Department of Obstetrics & Gynaecology, University of Toronto, Toronto, Ontario, Canada.
Melbourne School of Population & Global Health, University of Melbourne, Melbourne, Victoria, Australia.
JAMA Netw Open. 2022 May 2;5(5):e2213521. doi: 10.1001/jamanetworkopen.2022.13521.
Physicians may be at risk of pregnancy complications due to prolonged work hours, overnight shifts, occupational hazards, and older maternal age at first birth compared with nonphysicians. Observational studies of physicians, including comparisons across physician specialties, are needed.
To compare adverse maternal and perinatal outcomes between pregnant physicians and nonphysicians and between physicians of different specialties.
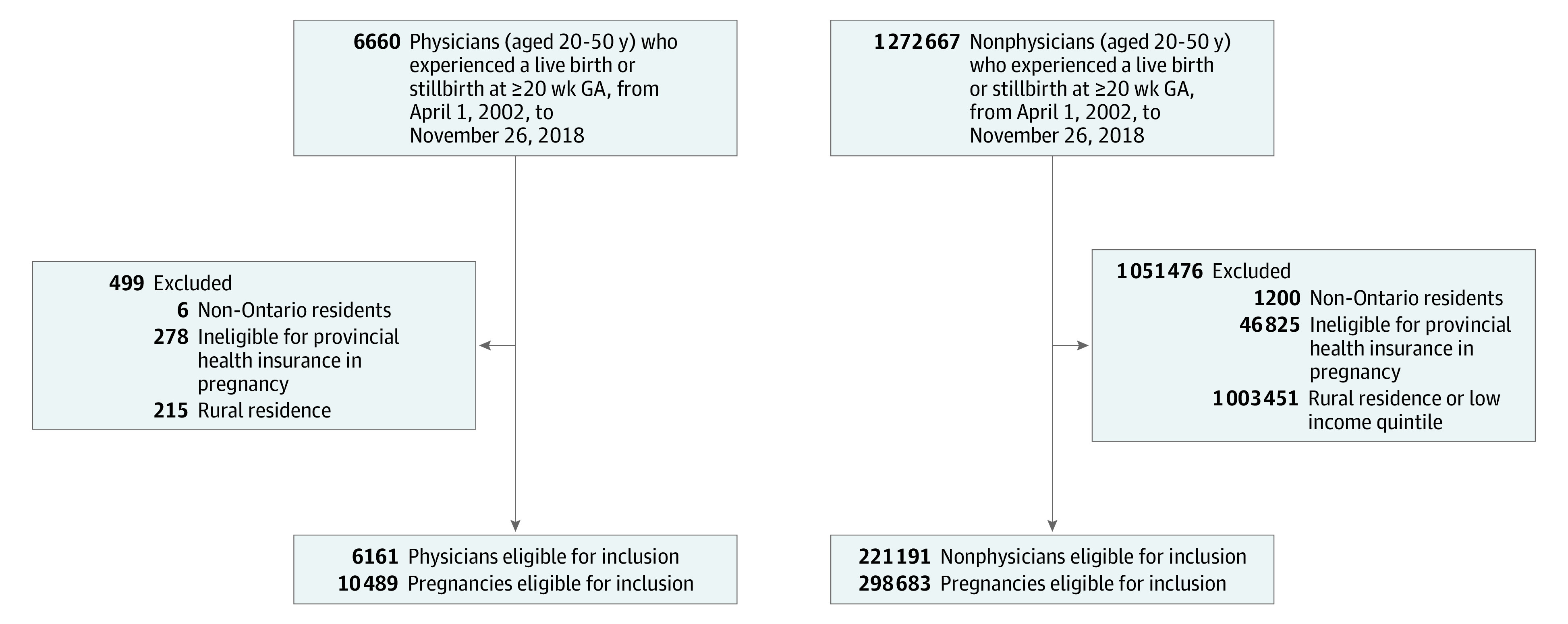
DESIGN, SETTING, AND PARTICIPANTS: A population-based retrospective cohort study was conducted in Ontario, Canada. Participants included physicians and nonphysician comparators residing in high-income areas who experienced a birth at 20 or more weeks' gestation from April 1, 2002, to November 26, 2018. Data analysis was performed from December 2020 to March 2022.
Physician occupation and physician specialty.
Severe maternal morbidity (in pregnancy and up to 42 days' post partum) and severe neonatal morbidity (up to hospital discharge among live-born infants) were the primary outcomes. Logistic regression under a generalized estimating equations approach was used to compare outcomes between physicians and nonphysicians, accounting for potentially more than 1 pregnancy per woman. Odds ratios were adjusted (aOR) for maternal age, parity, previous preterm birth, calendar year, immigration status, comorbidities, multiple gestation, and mode of delivery.
A total of 10 489 births occurred among 6161 licensed physicians, and 298 683 births occurred among 211 191 nonphysician counterparts. Physicians were older (median [IQR] age, 34 [31-36] vs 32 [29-35] years) and more likely to be nulliparous (5049 [48.1%] vs 128 961 [43.2%]) compared with nonphysicians. Severe maternal morbidity was more likely to occur among physicians than nonphysicians (unadjusted OR, 1.21; 95% CI, 1.04-1.41) but not after adjusting for study covariates (aOR, 1.13; 95% CI, 0.97-1.32). Severe neonatal morbidity was less likely to occur among infants of physicians than infants of nonphysicians (aOR, 0.79; 95% CI, 0.72-0.87). Compared with family physicians, neither nonsurgical specialists (aOR, 1.12; 95% CI, 0.82-1.53) nor surgical specialists (aOR, 1.43; 95% CI, 0.74-2.76) were at increased risk of severe maternal morbidity. Similar findings were observed for severe neonatal morbidity (nonsurgical specialists: aOR, 0.98; 95% CI, 0.80-1.19; surgical specialists: aOR, 1.08; 95% CI, 0.68-1.71).
The findings of this study suggest that female physicians may be at slightly higher risk of severe maternal morbidity. This association appeared to be mediated by their tendency to delay childbearing compared with nonphysicians. Newborns of physicians appear to experience less morbidity. Such differences were not observed between physician specialty groups.
与非医师相比,由于工作时间延长、值夜班、职业危害以及初次生育时母亲年龄较大,医生可能面临妊娠并发症的风险。需要进行包括比较不同医师专业的医师观察性研究。
比较孕妇医生和非医生以及不同专业医生之间的不良母婴和围产结局。
设计、地点和参与者:这是一项在加拿大安大略省进行的基于人群的回顾性队列研究。参与者包括居住在高收入地区的 20 周或以上妊娠分娩的医生和非医生比较者。数据分析于 2020 年 12 月至 2022 年 3 月进行。
医生职业和医生专业。
严重的母体发病率(妊娠和产后 42 天内)和严重的新生儿发病率(活产儿的住院期间)是主要结局。使用广义估计方程方法下的逻辑回归来比较医生和非医生之间的结果,每个女性可能有超过一次的妊娠。优势比(aOR)经产妇年龄、产次、既往早产、日历年份、移民身份、合并症、多胎妊娠和分娩方式进行调整。
在 6161 名持照医生中,共有 10489 名分娩,在 211191 名非医生同行中,共有 298683 名分娩。与非医生相比,医生年龄较大(中位数[IQR]年龄,34 [31-36]岁与 32 [29-35]岁)且更可能是初产妇(5049 [48.1%]与 128961 [43.2%])。与非医生相比,医生发生严重母体发病率的可能性更高(未调整的 OR,1.21;95%CI,1.04-1.41),但在调整研究协变量后(aOR,1.13;95%CI,0.97-1.32)并非如此。与非医生相比,医生的新生儿严重发病率较低(aOR,0.79;95%CI,0.72-0.87)。与家庭医生相比,非外科专家(aOR,1.12;95%CI,0.82-1.53)和外科专家(aOR,1.43;95%CI,0.74-2.76)均未增加严重母体发病率的风险。对于严重新生儿发病率,也观察到类似的发现(非外科专家:aOR,0.98;95%CI,0.80-1.19;外科专家:aOR,1.08;95%CI,0.68-1.71)。
这项研究的结果表明,女性医生可能面临更高的严重母体发病率风险。这种关联似乎是由于与非医生相比,她们倾向于延迟生育。医生的新生儿似乎发病率较低。在医师专业群体之间没有观察到这种差异。