Department of Neurosurgery, Xiangya Hospital, Central South University, Changsha, Hunan, China.
Hypothalamic Pituitary Research Centre, Xiangya Hospital, Central South University, Changsha, China.
BMJ. 2022 May 25;377:e067946. doi: 10.1136/bmj-2021-067946.
To investigate the association between gestational diabetes mellitus and adverse outcomes of pregnancy after adjustment for at least minimal confounding factors.
Systematic review and meta-analysis.
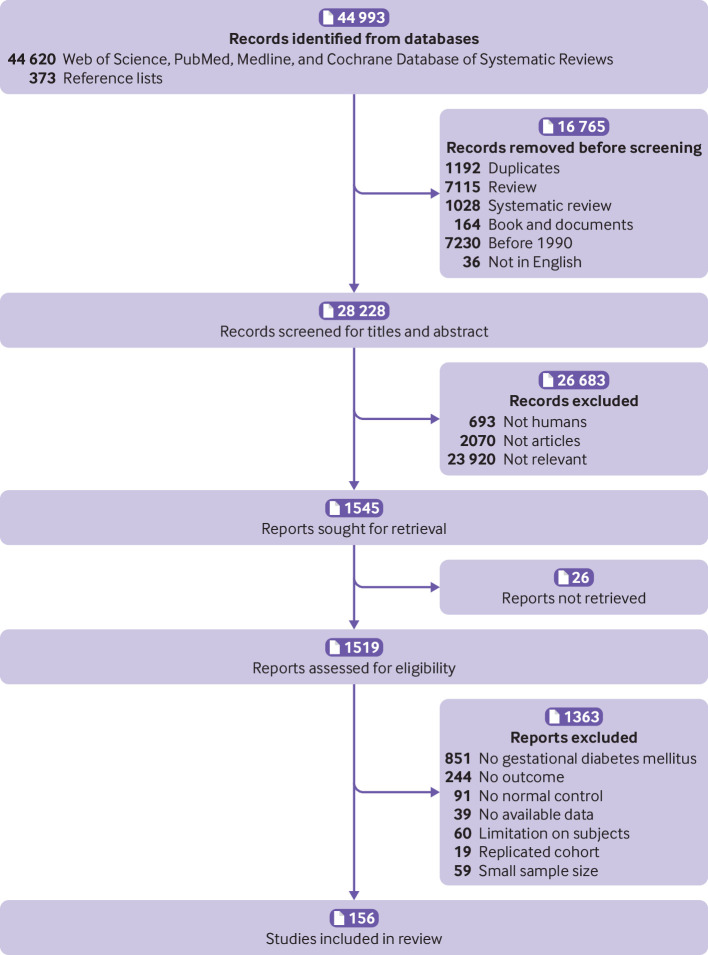
Web of Science, PubMed, Medline, and Cochrane Database of Systematic Reviews, from 1 January 1990 to 1 November 2021.
Cohort studies and control arms of trials reporting complications of pregnancy in women with gestational diabetes mellitus were eligible for inclusion. Based on the use of insulin, studies were divided into three subgroups: no insulin use (patients never used insulin during the course of the disease), insulin use (different proportions of patients were treated with insulin), and insulin use not reported. Subgroup analyses were performed based on the status of the country (developed or developing), quality of the study, diagnostic criteria, and screening method. Meta-regression models were applied based on the proportion of patients who had received insulin.
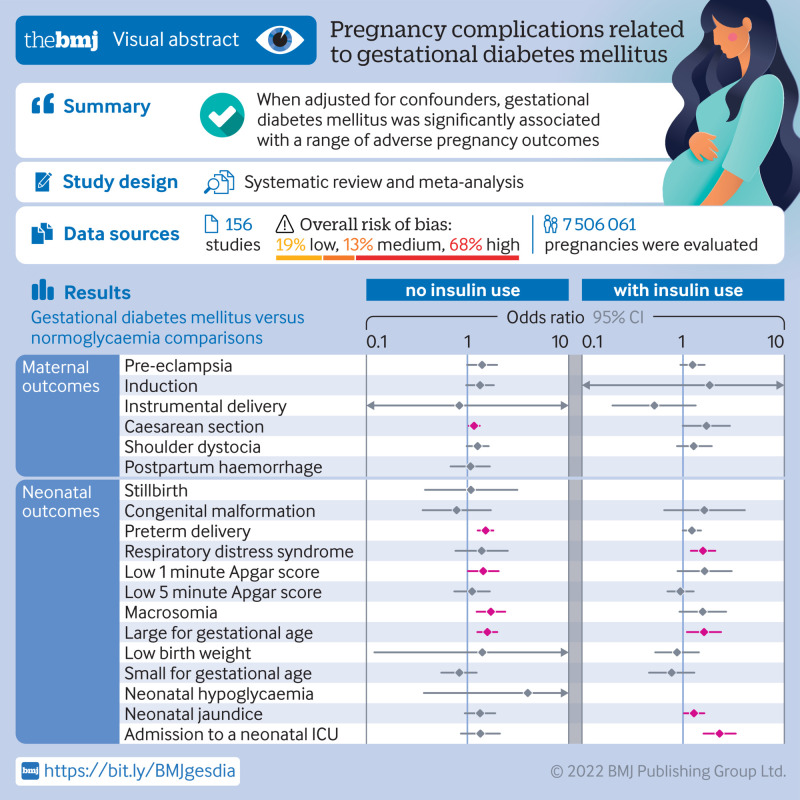
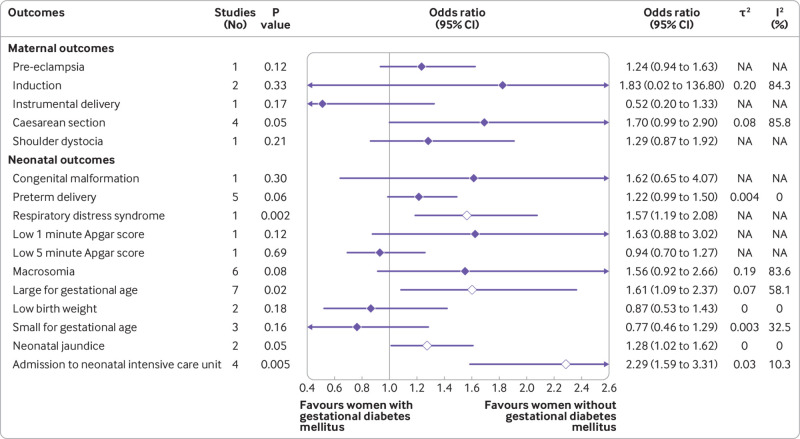
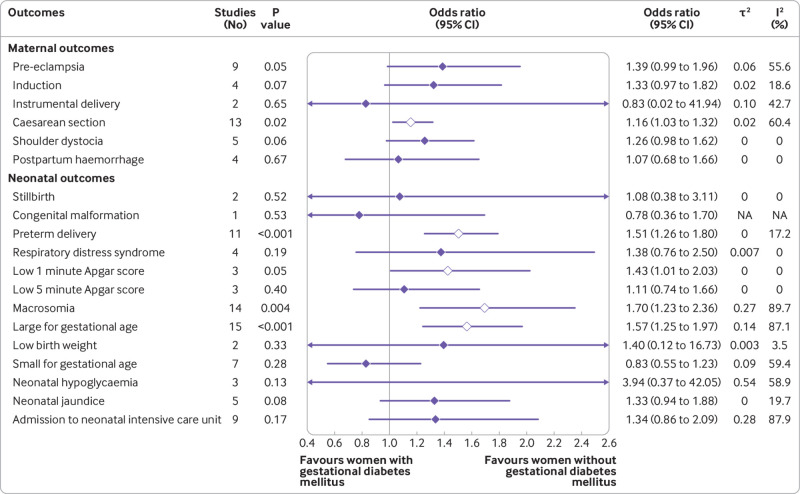
156 studies with 7 506 061 pregnancies were included, and 50 (32.1%) showed a low or medium risk of bias. In studies with no insulin use, when adjusted for confounders, women with gestational diabetes mellitus had increased odds of caesarean section (odds ratio 1.16, 95% confidence interval 1.03 to 1.32), preterm delivery (1.51, 1.26 to 1.80), low one minute Apgar score (1.43, 1.01 to 2.03), macrosomia (1.70, 1.23 to 2.36), and infant born large for gestational age (1.57, 1.25 to 1.97). In studies with insulin use, when adjusted for confounders, the odds of having an infant large for gestational age (odds ratio 1.61, 1.09 to 2.37), or with respiratory distress syndrome (1.57, 1.19 to 2.08) or neonatal jaundice (1.28, 1.02 to 1.62), or requiring admission to the neonatal intensive care unit (2.29, 1.59 to 3.31), were higher in women with gestational diabetes mellitus than in those without diabetes. No clear evidence was found for differences in the odds of instrumental delivery, shoulder dystocia, postpartum haemorrhage, stillbirth, neonatal death, low five minute Apgar score, low birth weight, and small for gestational age between women with and without gestational diabetes mellitus after adjusting for confounders. Country status, adjustment for body mass index, and screening methods significantly contributed to heterogeneity between studies for several adverse outcomes of pregnancy.
When adjusted for confounders, gestational diabetes mellitus was significantly associated with pregnancy complications. The findings contribute to a more comprehensive understanding of the adverse outcomes of pregnancy related to gestational diabetes mellitus. Future primary studies should routinely consider adjusting for a more complete set of prognostic factors.
PROSPERO CRD42021265837.
在调整至少最小混杂因素后,研究妊娠期糖尿病与妊娠不良结局之间的关联。
系统评价和荟萃分析。
Web of Science、PubMed、Medline 和 Cochrane 系统评价数据库,时间范围为 1990 年 1 月 1 日至 2021 年 11 月 1 日。
纳入了报告妊娠期糖尿病患者妊娠并发症的队列研究和试验的对照臂。根据胰岛素的使用情况,研究分为三组:未使用胰岛素(患者在疾病过程中从未使用过胰岛素)、使用胰岛素(不同比例的患者接受胰岛素治疗)和未报告胰岛素使用情况。根据国家(发达国家或发展中国家)、研究质量、诊断标准和筛查方法的情况进行亚组分析。根据接受胰岛素治疗的患者比例,应用了元回归模型。
纳入了 156 项研究,共涉及 7506061 例妊娠,其中 50 项(32.1%)研究存在低或中风险偏倚。在未使用胰岛素的研究中,调整混杂因素后,妊娠期糖尿病患者剖宫产(比值比 1.16,95%置信区间 1.03 至 1.32)、早产(1.51,1.26 至 1.80)、1 分钟 Apgar 评分低(1.43,1.01 至 2.03)、巨大儿(1.70,1.23 至 2.36)和婴儿出生时大于胎龄(1.57,1.25 至 1.97)的风险增加。在使用胰岛素的研究中,调整混杂因素后,妊娠期糖尿病患者的巨大儿(比值比 1.61,1.09 至 2.37)、呼吸窘迫综合征(1.57,1.19 至 2.08)或新生儿黄疸(1.28,1.02 至 1.62)、或需要入住新生儿重症监护病房(2.29,1.59 至 3.31)的风险高于无糖尿病的患者。调整混杂因素后,未发现妊娠期糖尿病患者与无糖尿病患者在器械分娩、肩难产、产后出血、死胎、新生儿死亡、5 分钟 Apgar 评分低、低出生体重和小于胎龄儿等不良妊娠结局的风险存在差异。国家地位、调整体重指数和筛查方法对几项妊娠不良结局的研究间异质性有显著贡献。
在调整混杂因素后,妊娠期糖尿病与妊娠并发症显著相关。这些发现有助于更全面地了解与妊娠期糖尿病相关的妊娠不良结局。未来的原始研究应常规考虑调整更完整的预后因素。
PROSPERO CRD42021265837。