Steurer Martina A, Tonna Joseph E, Coyan Garrett N, Burki Sarah, Sciortino Christopher M, Oishi Peter E
Division of Pediatric Critical Care Medicine, Department of Pediatrics, University of California, San Francisco, San Francisco, CA.
Department of Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, CA.
Crit Care Explor. 2022 May 16;4(5):e0698. doi: 10.1097/CCE.0000000000000698. eCollection 2022 May.
We aimed to investigate whether there are differences in outcome for pediatric patients when extracorporeal life support (ECLS) is initiated on-hours compared with off-hours.
Retrospective cohort study.
Ten-year period (2009-2018) in United States centers, from the Extracorporeal Life Support Organization registry.
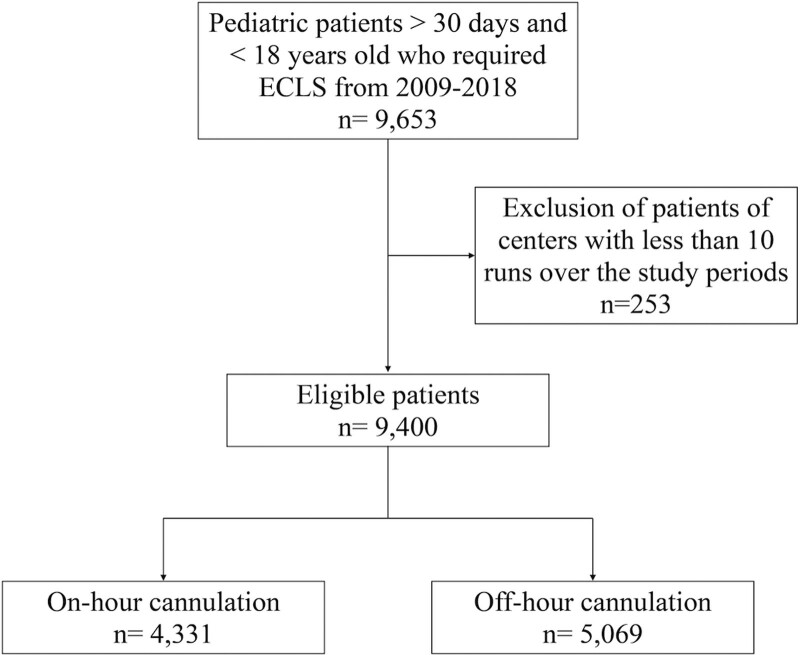
Pediatric (>30 d and <18 yr old) patients undergoing venovenous and venoarterial ECLS.
The primary predictor was on versus off-hours cannulation. On-hours were defined as 0700-1859 from Monday to Friday. Off-hours were defined as 1900-0659 from Monday to Thursday or 1900 Friday to 0659 Monday or any time during a United States national holiday. The primary outcome was inhospital mortality. The secondary outcomes were complications related to ECLS and length of hospital stay.
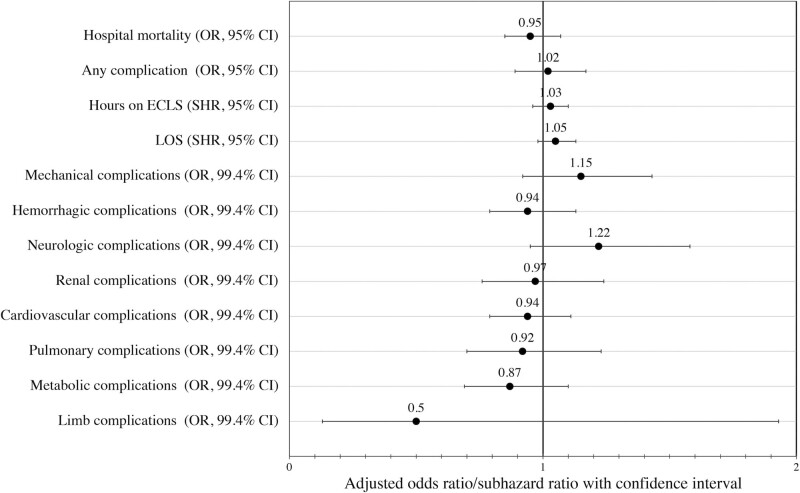
In a cohort of 9,400 patients, 4,331 (46.1%) were cannulated on-hours and 5,069 (53.9%) off-hours. In the off-hours group, 2,220/5,069 patients died (44.0%) versus 1,894/4,331 (44.1%) in the on-hours group ( = 0.93). Hemorrhagic complications were lower in the off-hours group versus the on-hours group (hemorrhagic 18.4% vs 21.0%; = 0.002). After adjusting for patient complexity and other confounders, there were no differences between the groups in mortality (odds ratio [OR], 0.95; 95% CI, 0.85-1.07; = 0.41) or any complications (OR, 1.02; 95% CI, 0.89-1.17; = 0.75).
Survival and complication rates are similar for pediatric patients when ECLS is initiated on-hours compared with off-hours. This finding suggests that, in aggregate, the current pediatric ECLS infrastructure in the United States provides adequate capabilities for the initiation of ECLS across all hours of the day.
我们旨在调查小儿患者在非工作时间与工作时间开始接受体外生命支持(ECLS)时,其治疗结果是否存在差异。
回顾性队列研究。
美国各中心为期十年(2009 - 2018年)的数据,来源于体外生命支持组织登记处。
接受静脉 - 静脉和静脉 - 动脉ECLS治疗的儿科患者(年龄>30天且<18岁)。
主要预测因素是工作时间与非工作时间插管。工作时间定义为周一至周五的07:00 - 18:59。非工作时间定义为周一至周四的19:00 - 06:59、周五的19:00至周一的06:59或美国法定节假日的任何时间。主要结局是住院死亡率。次要结局是与ECLS相关的并发症和住院时间。
在9400例患者队列中,4331例(46.1%)在工作时间插管,5069例(53.9%)在非工作时间插管。在非工作时间组中,2220/5069例患者死亡(44.0%),而工作时间组为1894/4331例(44.1%)(P = 0.93)。非工作时间组的出血并发症低于工作时间组(出血并发症发生率分别为18.4%和21.0%;P = 0.002)。在对患者复杂性和其他混杂因素进行调整后,两组在死亡率(优势比[OR],0.95;95%置信区间[CI],0.85 - 1.07;P = 0.41)或任何并发症方面(OR,1.02;95% CI,0.89 - 1.17;P = 0.75)均无差异。
小儿患者在工作时间与非工作时间开始接受ECLS时,生存率和并发症发生率相似。这一发现表明,总体而言,美国目前的儿科ECLS基础设施能够在一天中的所有时间提供足够的ECLS启动能力。