Falette Puisieux Manon, Pellat Anna, Assaf Antoine, Ginestet Claire, Brezault Catherine, Dhooge Marion, Soyer Philippe, Coriat Romain
Gastroenterology and Digestive Oncology Unit, Cochin Hospital, AP-HP Centre, 27 Rue du Faubourg Saint-Jacques, 75014 Paris, France.
Faculté de Médecine, Université Paris Cité, 75006 Paris, France.
Cancers (Basel). 2022 May 10;14(10):2357. doi: 10.3390/cancers14102357.
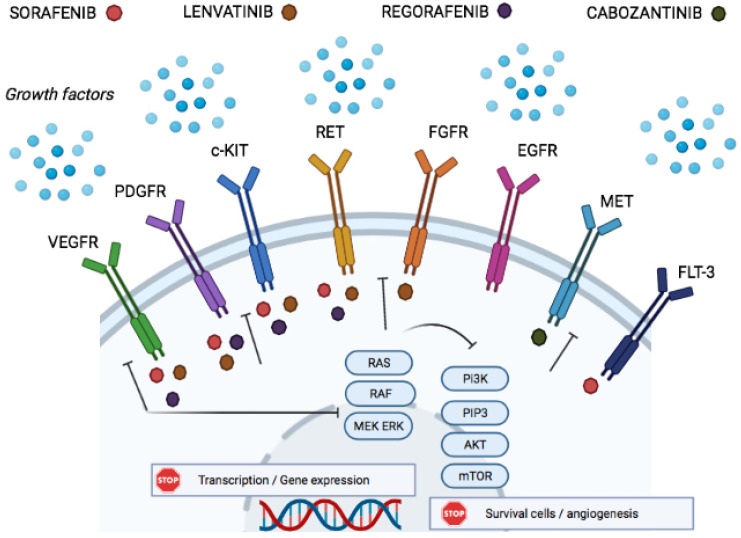
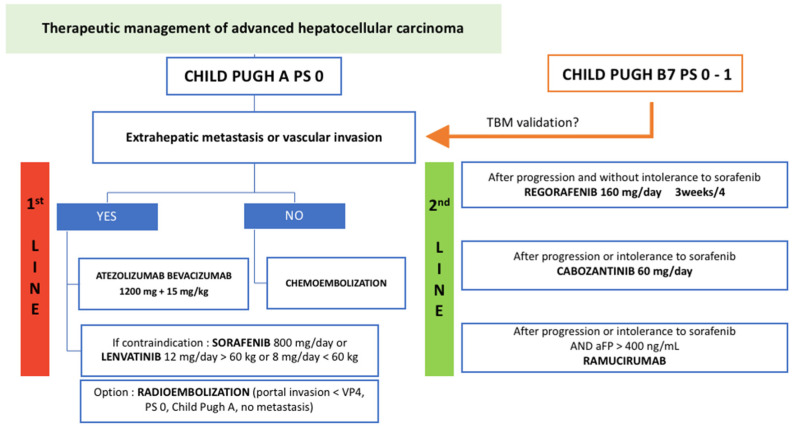
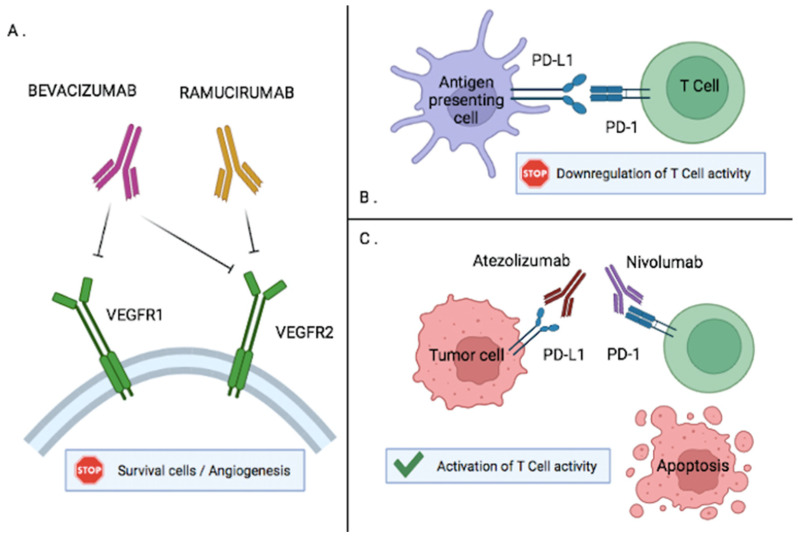
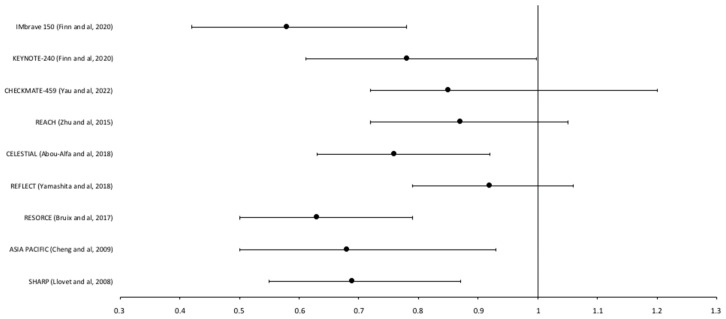
Hepatocellular carcinoma (HCC) usually occurs in the setting of liver cirrhosis and more rarely in a healthy liver. Its incidence has increased in the past years, especially in western countries with the rising prevalence of non-alcoholic fatty liver disease. The prognosis of advanced HCC is low. In the first-line setting of advanced HCC, sorafenib, a tyrosine kinase inhibitor, was the only validated treatment for many years. In 2020, the combination of atezolizumab, an immune checkpoint inhibitor, and bevacizumab showed superiority to sorafenib alone in survival, making it the first-line recommended treatment. Regorafenib and lenvatinib, other multikinase inhibitors, were also validated in the second and first-line settings, respectively. Transarterial chemoembolization can be an alternative treatment for patients with intermediate-stage HCC and preserved liver function, including unresectable multinodular HCC without extrahepatic spread. The current challenge in advanced HCC lies in the selection of a patient for the optimal treatment, taking into account the underlying liver disease and liver function. Indeed, all trial patients present with a Child-Pugh score of A, and the optimal approach for other patients is still unclear. Furthermore, the combination of atezolizumab and bevacizumab should be considered in the absence of medical contraindication. Many trials testing immune checkpoint inhibitors in association with anti-angiogenic agents are ongoing, and primary results are promising. The landscape in advanced HCC management is undergoing profound change, and many challenges remain for optimal patient management in the years to come. This review aimed to provide an overview of current systemic treatment options for patients with advanced unresectable HCC who are not candidates for liver-directed therapy.
肝细胞癌(HCC)通常发生在肝硬化背景下,在健康肝脏中则较为罕见。在过去几年中,其发病率有所上升,尤其是在非酒精性脂肪性肝病患病率不断上升的西方国家。晚期HCC的预后较差。在晚期HCC的一线治疗中,多年来索拉非尼(一种酪氨酸激酶抑制剂)是唯一经过验证的治疗方法。2020年,免疫检查点抑制剂阿替利珠单抗与贝伐单抗联合使用在生存期方面显示出优于单独使用索拉非尼,使其成为一线推荐治疗方法。瑞戈非尼和乐伐替尼这两种其他多激酶抑制剂也分别在二线和一线治疗中得到验证。经动脉化疗栓塞可作为肝功能良好的中期HCC患者的替代治疗方法,包括无法切除且无肝外转移的多结节HCC。晚期HCC目前面临的挑战在于,要考虑潜在的肝脏疾病和肝功能,为患者选择最佳治疗方案。实际上,所有试验患者的Child-Pugh评分为A级,而其他患者的最佳治疗方法仍不明确。此外,在没有医学禁忌证的情况下应考虑使用阿替利珠单抗和贝伐单抗联合治疗。许多测试免疫检查点抑制剂与抗血管生成药物联合使用的试验正在进行,初步结果很有前景。晚期HCC的治疗格局正在发生深刻变化,在未来几年中,优化患者管理仍面临许多挑战。本综述旨在概述目前针对无法切除的晚期HCC且不适合肝导向治疗的患者的全身治疗选择。