Kuo Yuan-Hung, Yen Yi-Hao, Chen Yen-Yang, Kee Kwong-Ming, Hung Chao-Hung, Lu Sheng-Nan, Hu Tsung-Hui, Chen Chien-Hung, Wang Jing-Houng
Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Division of Hematology-Oncology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Front Oncol. 2021 May 31;11:683341. doi: 10.3389/fonc.2021.683341. eCollection 2021.
Nivolumab and regorafenib are approved second-line therapies for patients with hepatocellular carcinoma (HCC) after sorafenib failure. This study compared the effectiveness of nivolumab and regorafenib following sorafenib.
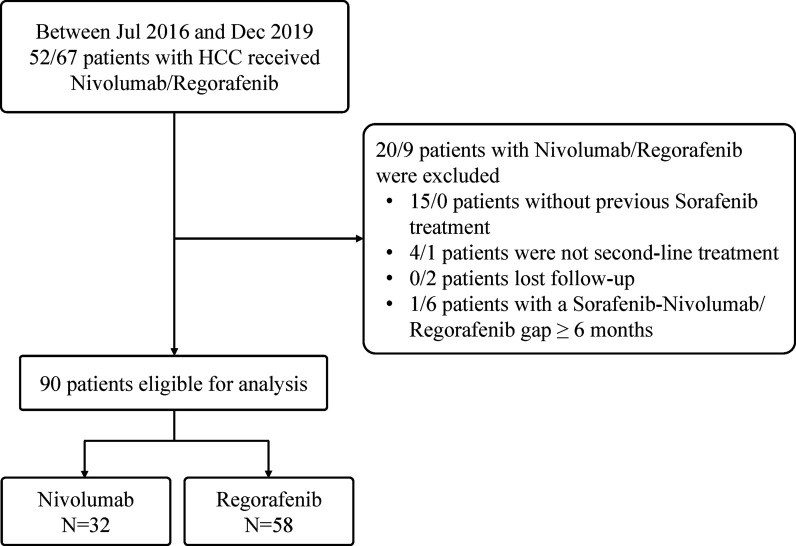
We retrospectively enrolled HCC patients who had undergone nivolumab or regorafenib after sorafenib failure. Treatment response, treatment-related adverse events (TRAE) and clinical outcomes of study patients were recorded and analyzed.
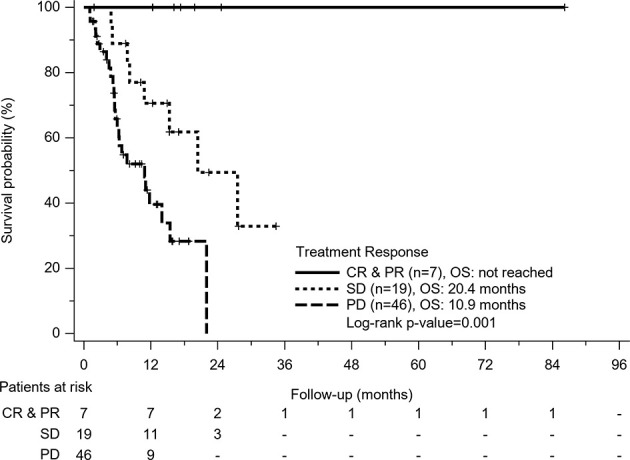
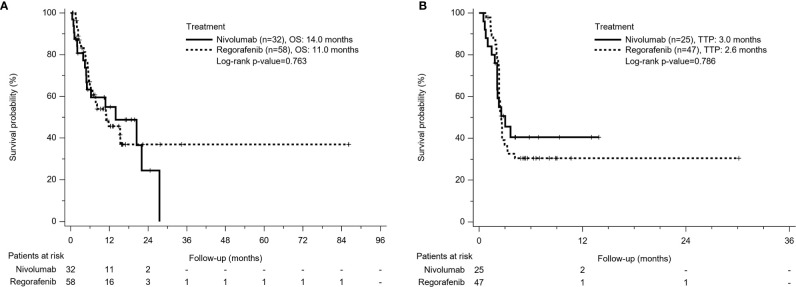
A total of 90 patients (male/female: 67/23, mean age: 63 years) were enrolled, including 32 patients in the Nivolumab group and 58 patients in the Regorafenib group. The Nivolumab group had better objective response rates (16% 6.4%) and disease control rates (44% 31.9%) than the Regorafenib group, but there was no statistical difference. The comparison of time to progression (3.0 months 2.6 months, p=0.786) and overall survival (OS) (14 months 11 months, p = 0.763) between Nivolumab and Regorafenib groups were also insignificant. Regarding number of TRAE incidences, the Nivolumab group was significantly lower than the Regorafenib group (37.5% 68%). After cession of nivolumab/regorafenib, 34 patients (37.8%) (Nivolumab group/Regorafenib group: 11/23) could afford the following therapies. Concerning sequential systemic therapies, 17 patients (18.9%) received third-line therapy, whereas six patients (6.7%) could move to fourth-line therapy. In multivariable analysis, patients who achieved disease control were associated with improved OS (hazard ratio, 0.18; 95% confidence interval, 0.07-0.46; p<0.001) after adjusting Child-Pugh class and post-treatment.
After sorafenib failure, using nivolumab or regorafenib both illustrated promising treatment outcomes.
纳武利尤单抗和瑞戈非尼是索拉非尼治疗失败后的肝细胞癌(HCC)患者获批的二线治疗方案。本研究比较了索拉非尼治疗后纳武利尤单抗和瑞戈非尼的疗效。
我们回顾性纳入了索拉非尼治疗失败后接受纳武利尤单抗或瑞戈非尼治疗的HCC患者。记录并分析研究患者的治疗反应、治疗相关不良事件(TRAE)和临床结局。
共纳入90例患者(男/女:67/23,平均年龄:63岁),其中纳武利尤单抗组32例,瑞戈非尼组58例。纳武利尤单抗组的客观缓解率(16% 对 6.4%)和疾病控制率(44% 对 31.9%)优于瑞戈非尼组,但无统计学差异。纳武利尤单抗组和瑞戈非尼组之间的疾病进展时间(3.0个月 对 2.6个月,p = 0.786)和总生存期(OS)(14个月 对 11个月,p = 0.763)比较也无显著差异。关于TRAE发生率,纳武利尤单抗组显著低于瑞戈非尼组(37.5% 对 68%)。停用纳武利尤单抗/瑞戈非尼后,34例患者(37.8%)(纳武利尤单抗组/瑞戈非尼组:11/23)能够接受后续治疗。关于序贯全身治疗,17例患者(18.9%)接受了三线治疗,而6例患者(6.7%)能够进入四线治疗。在多变量分析中,在调整Child-Pugh分级和治疗后,实现疾病控制的患者与改善的OS相关(风险比为0.18;95%置信区间为0.07 - 0.46;p < 0.001)。
索拉非尼治疗失败后,使用纳武利尤单抗或瑞戈非尼均显示出有前景的治疗结果。