Department of Anatomy, Institute of Biology, State University of Rio de Janeiro, Laboratory of Morphometry, Metabolism and Cardiovascular Diseases, Rio de Janeiro 20551-030, Brazil.
Department of Clinical and Toxicology Analysis, State University of Rio de Janeiro, Nutrition Institute, State University of Rio de Janeiro, Nutrition Institute, University of Sao Paulo, Rio de Janeiro 20551-030, Brazil.
World J Gastroenterol. 2022 May 7;28(17):1814-1829. doi: 10.3748/wjg.v28.i17.1814.
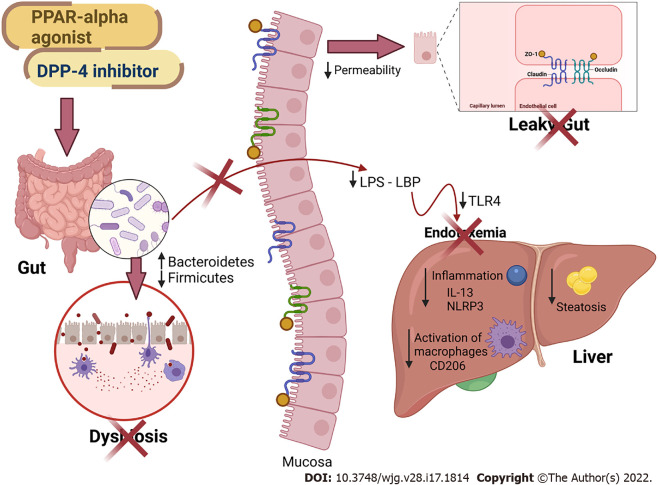
Obesity and comorbidities onset encompass gut dysbiosis, altered intestinal permeability, and endotoxemia. Treatments that target gut dysbiosis can cope with obesity and nonalcoholic fatty liver disease (NAFLD) management. Peroxisome proliferator-activated receptor (PPAR)-alpha activation and dipeptidyl-peptidase-4 (DPP-4) inhibition alleviate NAFLD, but the mechanism may involve gut microbiota modulation and merits further investigation.
To address the effects of PPAR-alpha activation and DPP-4 inhibition (isolated or combined) upon the gut-liver axis, emphasizing inflammatory pathways in NAFLD management in high-fat-fed C57BL/6J mice.
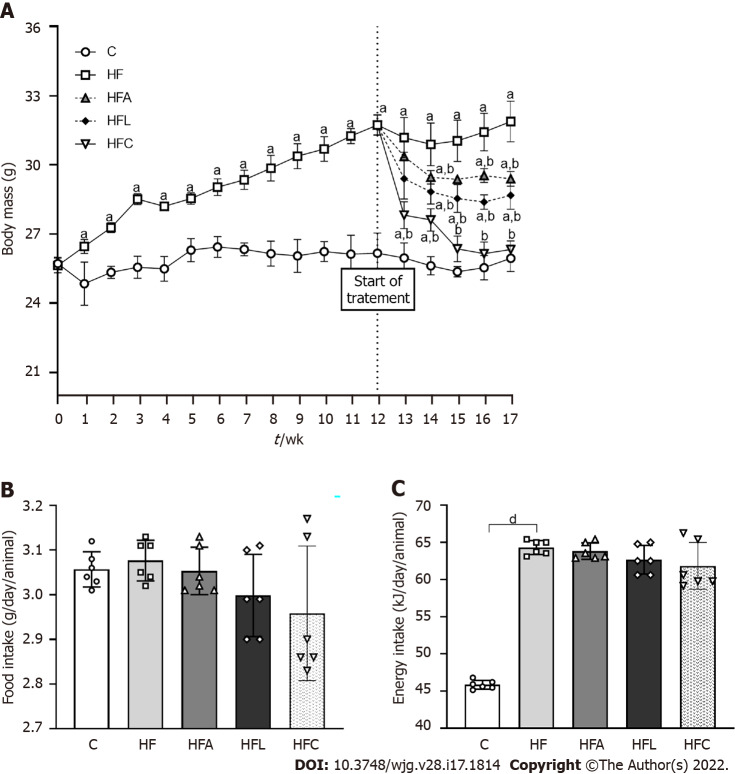
Male C57BL/6J mice were fed a control diet (C, 10% of energy as lipids) or a high-fat diet (HFD, 50% of energy as lipids) for 12 wk, when treatments started, forming the groups: C, HF, HFA (HFD + PPAR-alpha agonist WY14643, 2.5 mg/kg body mass), HFL (HFD + DPP-4 inhibitor linagliptin, 15 mg/kg body mass), and HFC (HFD + the combination of WY14643 and linagliptin).
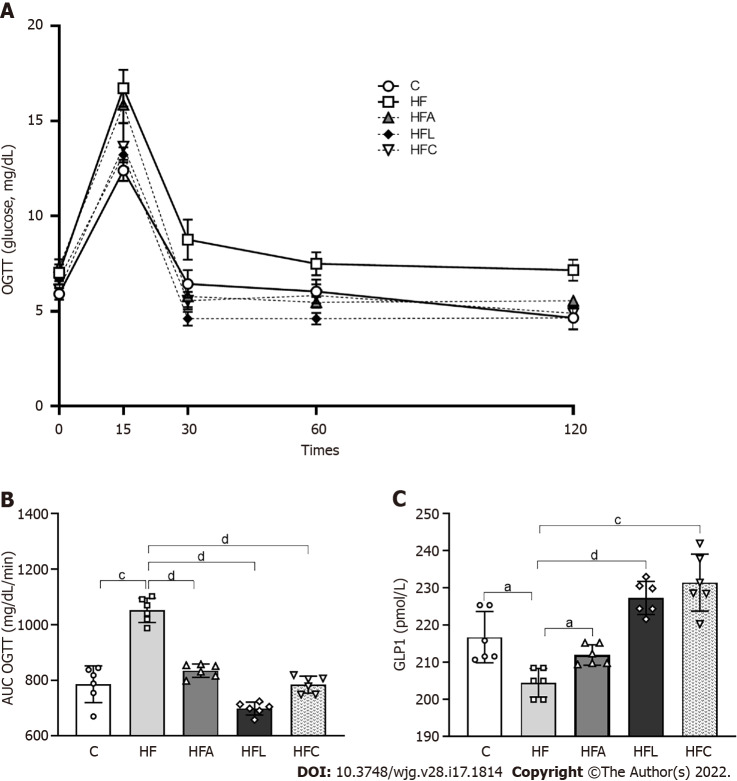
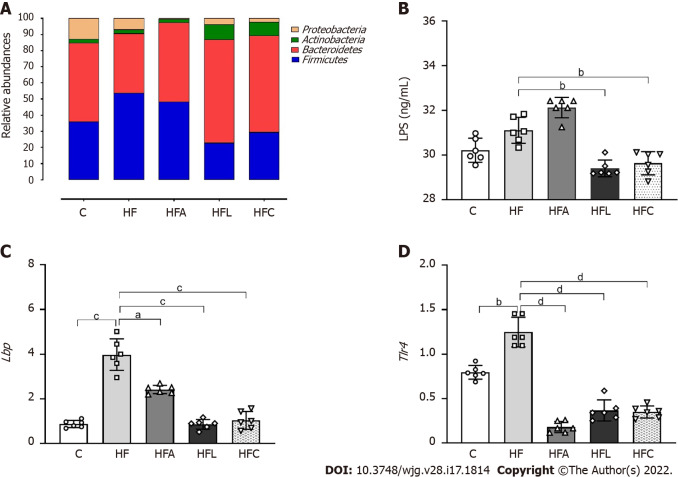
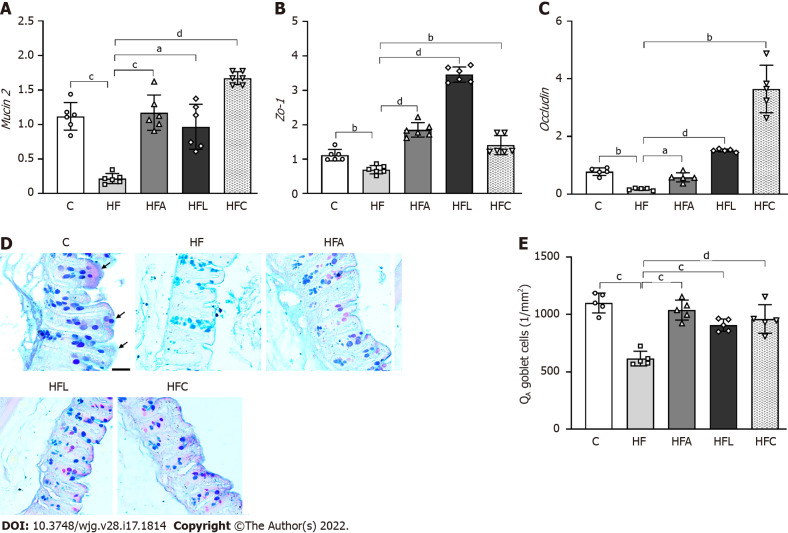
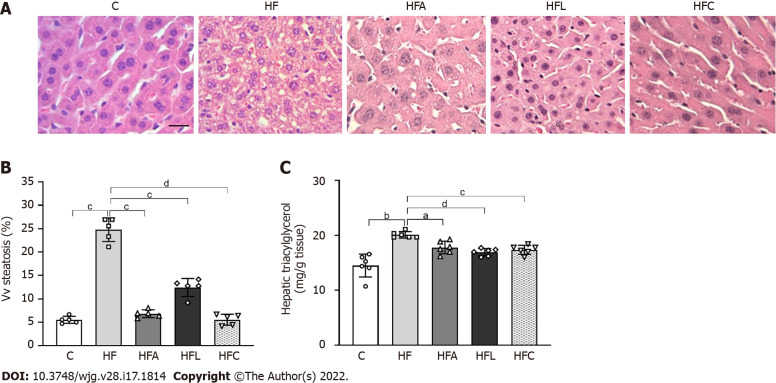
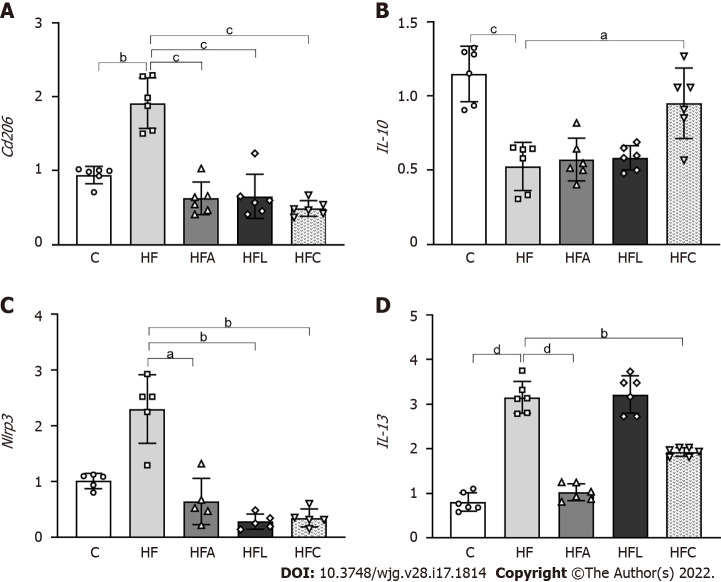
The HFD was obesogenic compared to the C diet. All treatments elicited significant body mass loss, and the HFC group showed similar body mass to the C group. All treatments tackled oral glucose intolerance and raised plasma glucagon-like peptide-1 concentrations. These metabolic benefits restored / ratio, resulting in increased goblet cells area of the large intestine and reduced lipopolysaccharides concentrations in treated groups. At the gene level, treated groups showed higher intestinal , , and expression than the HFD group. The reduced endotoxemia suppressed inflammasome and macrophage gene expression in the liver of treated animals. These observations complied with the mitigation of liver steatosis and reduced hepatic triacylglycerol, reassuring the role of the proposed treatments on NAFLD mitigation.
PPAR alpha activation and DPP-4 inhibition (isolated or combined) tackled NAFLD in diet-induced obese mice by restoration of gut-liver axis. The reestablishment of the intestinal barrier and the rescued phylogenetic gut bacteria distribution mitigated liver steatosis through anti-inflammatory signals. These results can cope with NAFLD management by providing pre-clinical evidence that drugs used to treat obesity comorbidities can help to alleviate this silent and harmful liver disease.
肥胖和合并症的发生包括肠道菌群失调、肠道通透性改变和内毒素血症。针对肠道菌群失调的治疗方法可以应对肥胖和非酒精性脂肪性肝病(NAFLD)的管理。过氧化物酶体增殖物激活受体(PPAR)-α激活和二肽基肽酶-4(DPP-4)抑制可缓解 NAFLD,但机制可能涉及肠道微生物群的调节,值得进一步研究。
探讨 PPAR-α激活和 DPP-4 抑制(单独或联合)对高脂肪喂养 C57BL/6J 小鼠肠道-肝脏轴的影响,强调在 NAFLD 管理中的炎症途径。
雄性 C57BL/6J 小鼠喂食对照饮食(C,10%能量来自脂肪)或高脂肪饮食(HFD,50%能量来自脂肪)12 周,当开始治疗时,形成以下组:C、HF、HFA(HFD+PPAR-α激动剂 WY14643,2.5mg/kg 体重)、HFL(HFD+DPP-4 抑制剂 linagliptin,15mg/kg 体重)和 HFC(HFD+WY14643 和 linagliptin 的联合治疗)。
与 C 饮食相比,HFD 具有致肥胖作用。所有治疗均显著减轻体重,HFC 组体重与 C 组相似。所有治疗均改善了口服葡萄糖耐量和升高了血浆胰高血糖素样肽-1 浓度。这些代谢益处恢复了 / 比值,导致大肠中的杯状细胞面积增加,处理组中的内毒素浓度降低。在基因水平上,与 HFD 组相比,处理组的肠道 、 和 表达更高。减少的内毒素血症抑制了处理动物肝脏中的炎症小体和巨噬细胞基因表达。这些观察结果与减轻肝脂肪变性和减少肝三酰甘油一致,证实了所提出的治疗方法对 NAFLD 缓解的作用。
PPARα激活和 DPP-4 抑制(单独或联合)通过恢复肠道-肝脏轴来治疗饮食诱导肥胖的小鼠的 NAFLD。肠道屏障的重建和肠道细菌分布的恢复通过抗炎信号减轻了肝脂肪变性。这些结果通过提供用于治疗肥胖合并症的药物可以帮助缓解这种沉默且有害的肝病的临床前证据,为 NAFLD 的管理提供了帮助。