Department of Medicine, College of Health Sciences, Makerere University, P.O. Box 7072, Kampala, Uganda.
Research Department, Infectious Diseases Institute, College of Health Sciences, Makerere University, Kampala, Uganda.
J Med Case Rep. 2022 May 31;16(1):214. doi: 10.1186/s13256-022-03436-1.
Human immunodeficiency virus/tuberculosis coinfections have amplified the multidrug-resistant tuberculosis pandemic in many countries in Sub-Saharan Africa, and multidrug-resistant tuberculosis has become a major public health threat. There is a paucity of data on severe complications of multidrug-resistant tuberculosis in the context of human immunodeficiency virus coinfection despite the increasing prevalence of multidrug-resistant tuberculosis/human immunodeficiency virus coinfection and the complexity of multidrug-resistant tuberculosis treatment. This report describes a rare case of complicated multidrug-resistant tuberculosis in a human immunodeficiency virus-positive individual.
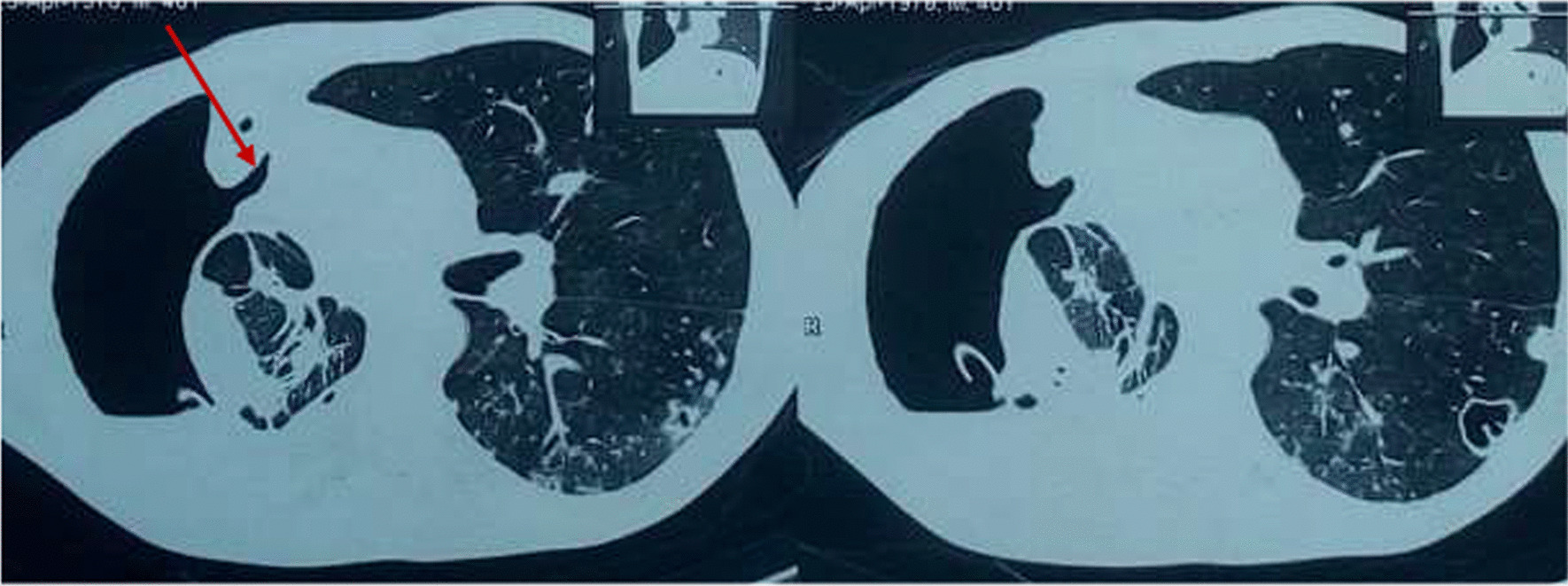
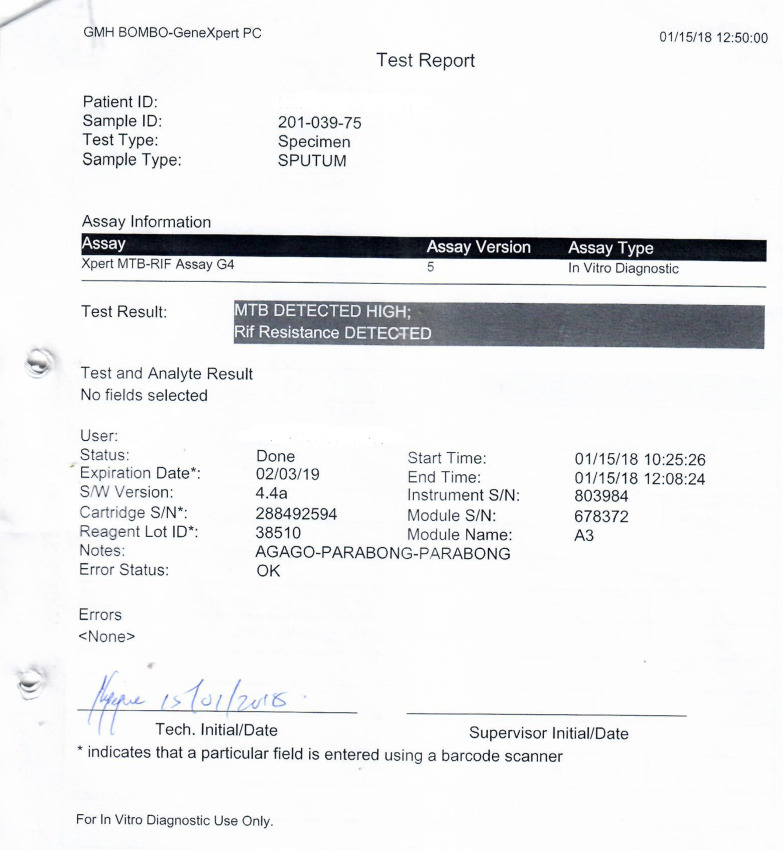
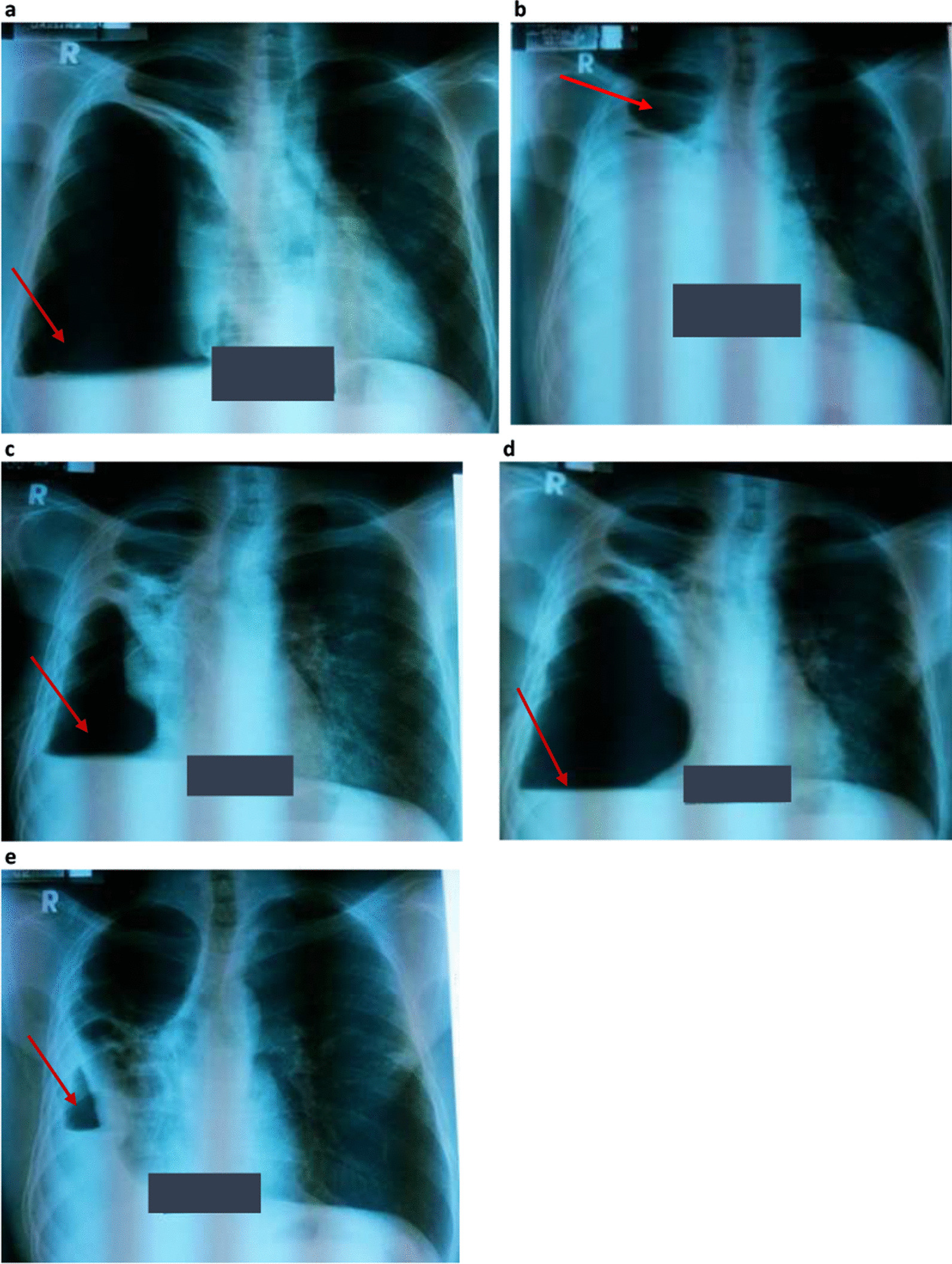
A 39-year-old human immunodeficiency virus-positive Ugandan male on anti-retroviral therapy for 6 years, who had recently completed treatment for drug-susceptible tuberculosis from a public hospital, presented to the tuberculosis ward of Mulago National Referral Hospital with worsening respiratory symptoms including persistent cough with purulent sputum, fever, right chest pain, and shortness of breath. On admission, a diagnosis of drug-resistant tuberculosis was made following a positive sputum Xpert MTB/Rif test with rifampicin resistance. Culture-based tuberculosis tests and line probe assay confirmed multidrug-resistant tuberculosis. The patient was given multidrug-resistant tuberculosis treatment that included bedaquiline, isoniazid, prothionamide, clofazimine, ethambutol, levofloxacin, and pyrazinamide and switched to second-line anti-retroviral therapy that included tenofovir/lamivudine/lopinavir/ritonavir. Chest X-ray revealed a hydro-pneumothorax, following which a chest tube was inserted. With persistent bubbling from the chest tube weeks later and a check chest X-ray that showed increasing pleural airspace (pneumothorax) and appearance of a new air-fluid level, chest computed tomography scan was performed, revealing a bronchopleural fistula in the right hemithorax. The computed tomography scan also revealed a pyo-pneumothorax and lung collapse involving the right middle and lower lobes as well as a thick-walled cavity in the right upper lobe. With the pulmonary complications, particularly the recurrent pneumothorax, bronchopleural fistula, and empyema thoracis, cardiothoracic surgeons were involved, who managed the patient conservatively and maintained the chest tube. The patient continued to be ill with recurrent pneumothorax despite the chest tube, until relatives opted for discharge against medical advice.
Complicated human immunodeficiency virus-related multidrug-resistant tuberculosis is not uncommon in settings of high human immunodeficiency virus/tuberculosis prevalence and is often associated with significant morbidity and mortality. Early diagnosis and treatment of multidrug-resistant tuberculosis, with rigorous monitoring for human immunodeficiency virus-positive individuals, is necessary to prevent debilitating complications.
人类免疫缺陷病毒/结核分枝杆菌合并感染使撒哈拉以南非洲许多国家的耐多药结核病大流行恶化,耐多药结核病已成为主要的公共卫生威胁。尽管耐多药结核分枝杆菌/人类免疫缺陷病毒合并感染的患病率不断增加,耐多药结核病的治疗也更加复杂,但合并人类免疫缺陷病毒感染的耐多药结核病严重并发症的数据仍然很少。本报告描述了一例人类免疫缺陷病毒阳性个体中罕见的耐多药结核病合并症病例。
一名 39 岁乌干达男性,人类免疫缺陷病毒阳性,接受抗逆转录病毒治疗 6 年,最近在公立医院完成了对药物敏感结核病的治疗,因呼吸症状恶化(包括持续咳嗽、脓性痰、发热、右侧胸痛和呼吸急促)而入住马鲁戈国家转诊医院的结核病房。入院时,由于 Xpert MTB/Rif 检测阳性且对利福平耐药,诊断为耐药结核病。培养结核病检测和线性探针分析证实为耐多药结核病。患者接受了耐多药结核病治疗,包括贝达喹啉、异烟肼、丙硫异烟胺、氯法齐明、乙胺丁醇、左氧氟沙星和吡嗪酰胺,并转为二线抗逆转录病毒治疗,包括替诺福韦/拉米夫定/洛匹那韦/利托那韦。胸部 X 射线显示为液气胸,随后插入胸腔引流管。数周后,引流管持续冒泡,复查胸部 X 射线显示胸腔气腔(气胸)增加,并出现新的液气平面,行胸部计算机断层扫描(CT)检查,显示右侧胸腔支气管胸膜瘘。CT 扫描还显示右侧中、下肺叶的脓气胸和肺塌陷,以及右上肺厚壁空洞。由于肺部并发症,特别是反复发作的气胸、支气管胸膜瘘和脓胸,心胸外科医生参与了治疗,他们对患者进行了保守治疗并保持了胸腔引流管的通畅。尽管有胸腔引流管,但患者仍持续病情恶化,反复发生气胸,直到家属选择违背医嘱出院。
在人类免疫缺陷病毒/结核病流行率高的环境中,与人类免疫缺陷病毒相关的耐多药结核病合并症并不少见,通常与显著的发病率和死亡率相关。早期诊断和治疗耐多药结核病,并对人类免疫缺陷病毒阳性个体进行严格监测,对于预防致残性并发症是必要的。