Epidemiology & Data Science, Amsterdam University Medical Centers, Vrije Universiteit, Amsterdam, The Netherlands
Rheumatology, Amsterdam Rheumatology and immunology Center, Amsterdam University Medical Centers, Vrije Universiteit, Amsterdam, The Netherlands.
Ann Rheum Dis. 2022 Jul;81(7):925-936. doi: 10.1136/annrheumdis-2021-221957. Epub 2022 May 31.
Low-dose glucocorticoid (GC) therapy is widely used in rheumatoid arthritis (RA) but the balance of benefit and harm is still unclear.
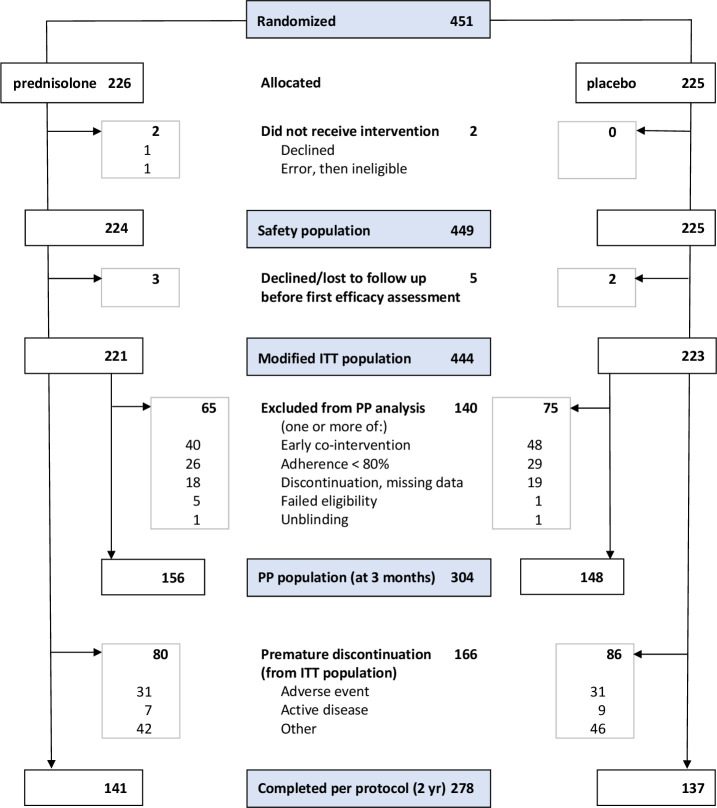
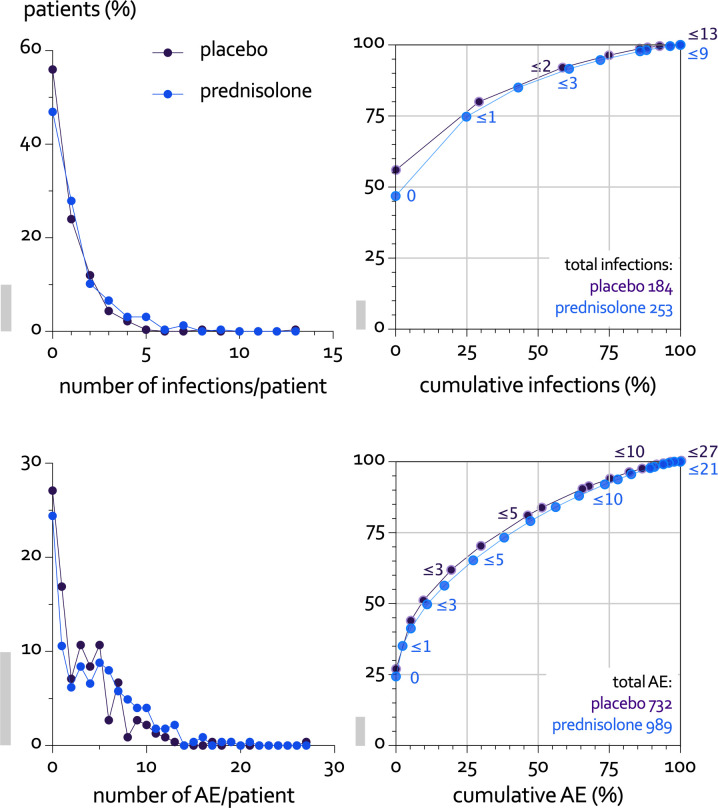
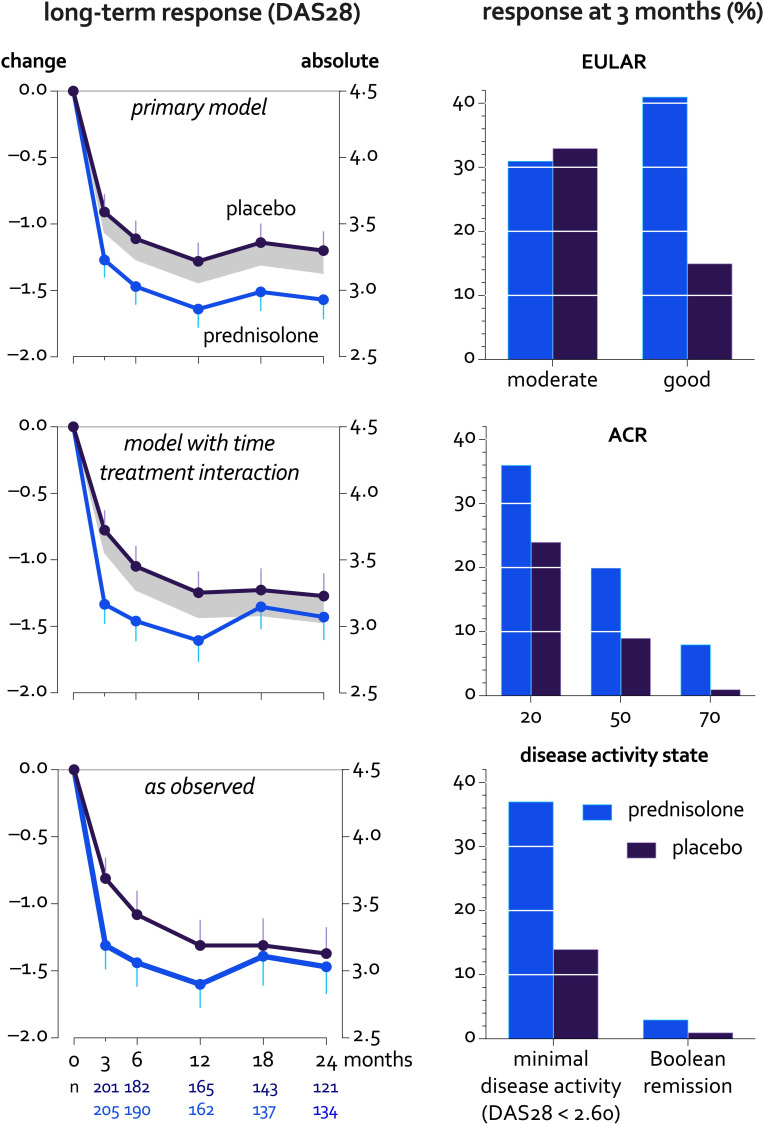
The GLORIA (Glucocorticoid LOw-dose in RheumatoId Arthritis) pragmatic double-blind randomised trial compared 2 years of prednisolone, 5 mg/day, to placebo in patients aged 65+ with active RA. We allowed all cotreatments except long-term open label GC and minimised exclusion criteria, tailored to seniors. Benefit outcomes included disease activity (disease activity score; DAS28, coprimary) and joint damage (Sharp/van der Heijde, secondary). The other coprimary outcome was harm, expressed as the proportion of patients with ≥1 adverse event (AE) of special interest. Such events comprised serious events, GC-specific events and those causing study discontinuation. Longitudinal models analysed the data, with one-sided testing and 95% confidence limits (95% CL).
We randomised 451 patients with established RA and mean 2.1 comorbidities, age 72, disease duration 11 years and DAS28 4.5. 79% were on disease-modifying treatment, including 14% on biologics. 63% prednisolone versus 61% placebo patients completed the trial. Discontinuations were for AE (both, 14%), active disease (3 vs 4%) and for other (including covid pandemic-related disease) reasons (19 vs 21%); mean time in study was 19 months. Disease activity was 0.37 points lower on prednisolone (95% CL 0.23, p<0.0001); joint damage progression was 1.7 points lower (95% CL 0.7, p=0.003). 60% versus 49% of patients experienced the harm outcome, adjusted relative risk 1.24 (95% CL 1.04, p=0.02), with the largest contrast in (mostly non-severe) infections. Other GC-specific events were rare.
Add-on low-dose prednisolone has beneficial long-term effects in senior patients with established RA, with a trade-off of 24% increase in patients with mostly non-severe AE; this suggests a favourable balance of benefit and harm.
NCT02585258.
小剂量糖皮质激素(GC)治疗被广泛用于类风湿关节炎(RA),但其获益与危害的平衡仍不明确。
GLORIA(糖皮质激素在老年类风湿关节炎中的低剂量)是一项实用的双盲随机试验,比较了 2 年泼尼松 5mg/天与安慰剂在 65 岁以上活动性 RA 患者中的疗效。我们允许使用所有伴随治疗(但不包括长期开放标签 GC),并根据老年人的特点量身定制了最小化排除标准。获益结局包括疾病活动度(疾病活动评分;DAS28,主要结局)和关节损伤(Sharp/van der Heijde,次要结局)。另一个主要结局是危害,用有≥1 个特殊关注不良事件(AE)的患者比例表示。这些事件包括严重事件、GC 特异性事件和导致研究中断的事件。纵向模型分析了数据,单侧检验和 95%置信区间(95%CI)。
我们共纳入了 451 例确诊 RA 且平均合并 2.1 种疾病的患者,年龄 72 岁,疾病病程 11 年,DAS28 4.5。79%的患者正在接受疾病修饰治疗,包括 14%的生物制剂治疗。451 例患者中,63%接受泼尼松治疗,61%接受安慰剂治疗,完成了试验。退出的原因是 AE(均为 14%)、疾病活动(3%比 4%)和其他原因(包括与新冠疫情相关的疾病)(19%比 21%);平均研究时间为 19 个月。泼尼松组的疾病活动度降低了 0.37 分(95%CI 0.23,p<0.0001);关节损伤进展降低了 1.7 分(95%CI 0.7,p=0.003)。60%的患者发生了危害结局,调整后的相对风险为 1.24(95%CI 1.04,p=0.02),主要是感染(大多为非严重感染)。其他 GC 特异性事件罕见。
在确诊的老年 RA 患者中,添加小剂量泼尼松有长期获益,与危害结局(AE)增加 24%相关,主要是发生非严重 AE;这表明获益与危害的平衡有利。
NCT02585258。