Crooke Philip S, Gattinoni Luciano, Michalik Michael, Marini John J
Department of Mathematics, Vanderbilt University, Nashville, TN, USA.
Department of Anesthesiology and Intensive Care, Gottingen University, Gottingen, Germany.
Intensive Care Med Exp. 2022 Jun 1;10(1):21. doi: 10.1186/s40635-022-00447-6.
Repeated expenditure of energy and its generation of damaging strain are required to injure the lung by ventilation (VILI). Mathematical modeling of passively inflated, single-compartment lungs with uniform parameters for resistance and compliance indicates that standard clinical modes (flow patterns) differ impressively with respect to the timing and intensity of energy delivery-the intracycle power (ICP) that determines parenchymal stress and strain. Although measures of elastic ICP may accurately characterize instantaneous rates of global energy delivery, how the ICP component delivered to a compartment affects the VILI-linked variable of strain is determined by compartmental mechanics, compartmental size and mode of gas delivery. We extended our one-compartment model of ICP to a multi-compartment setting that varied those characteristics.
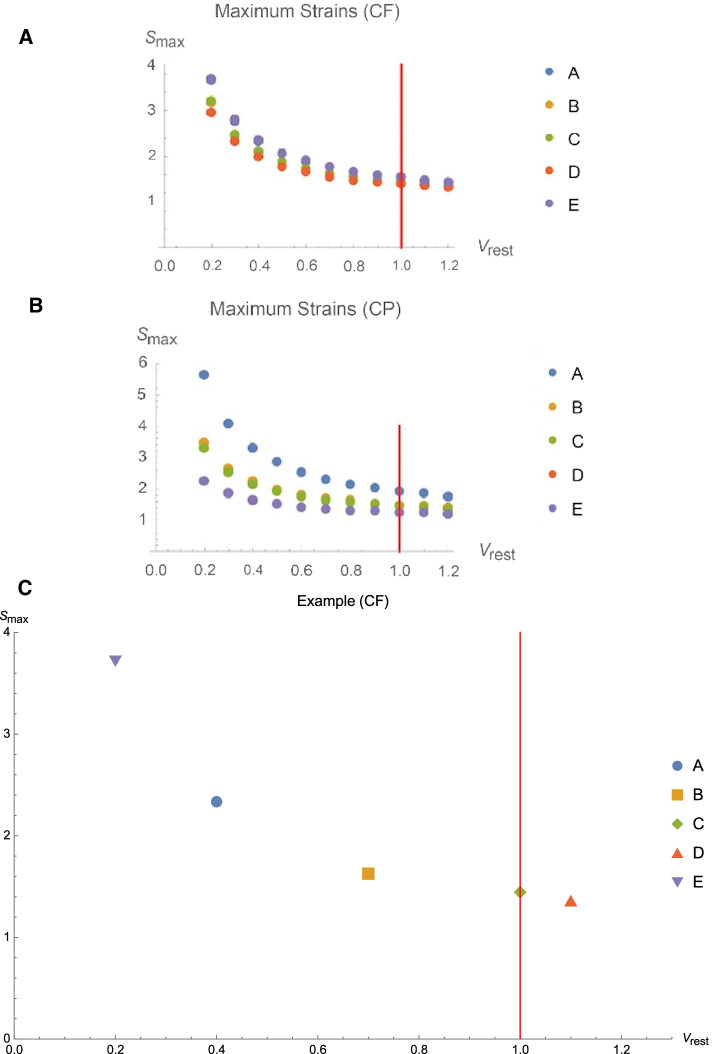
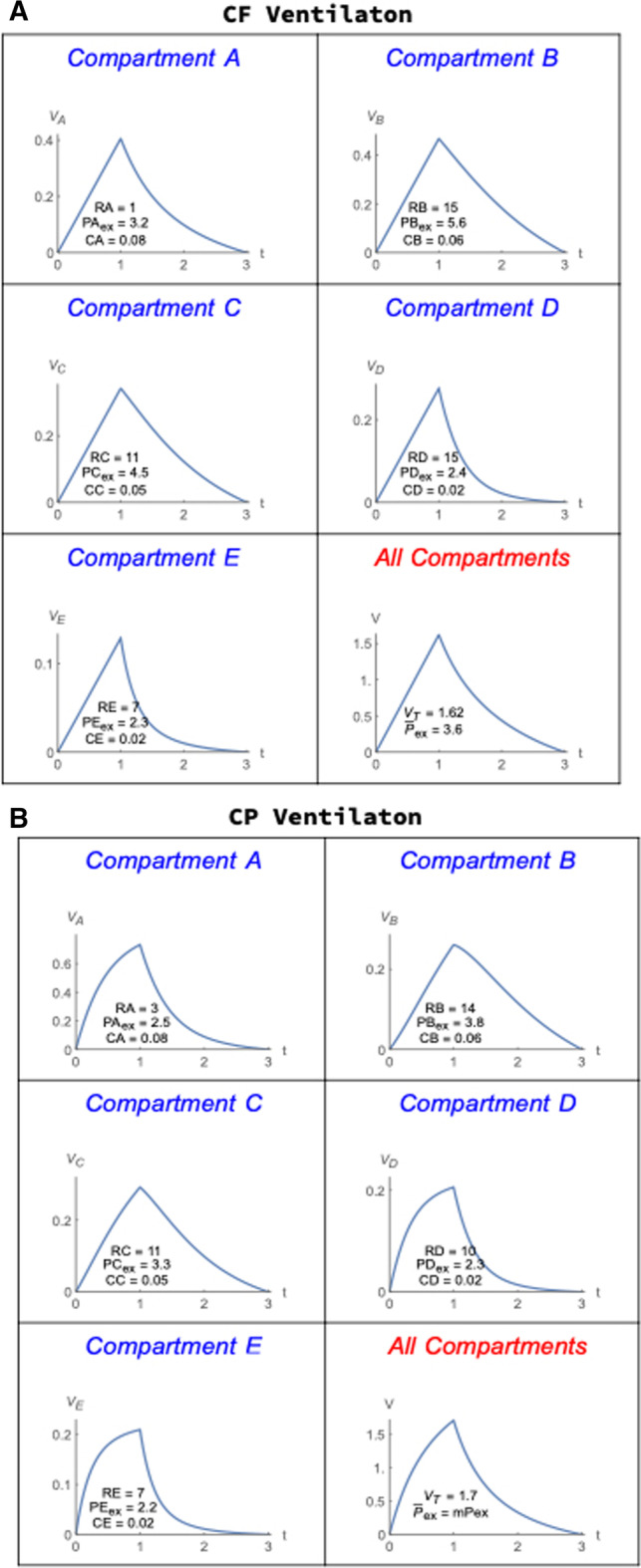
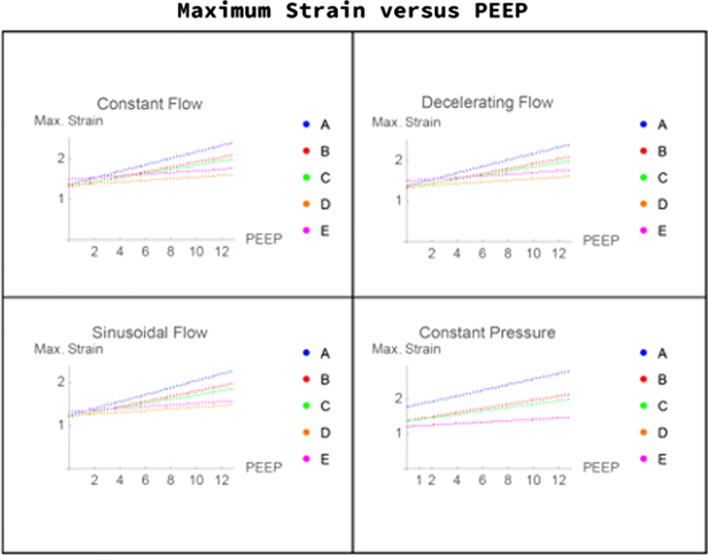
The primary findings of this model/simulation indicate that: (1) the strain and strain rate experienced within a modeled compartment are nonlinear functions of delivered energy and power, respectively; (2) for a given combination of flow profile and tidal volume, resting compartmental volumes influence their resulting maximal strains in response to breath delivery; (3) flow profile is a key determinant of the maximal strain as well as maximal strain rate experienced within a multi-compartment lung. By implication, different clinician-selected flow profiles not only influence the timing of power delivery, but also spatially distribute the attendant strains of expansion among compartments with diverse mechanical properties. Importantly, the contours and magnitudes of the compartmental ICP, strain, and strain rate curves are not congruent; strain and strain rate do not necessarily follow the compartmental ICP, and the hierarchy of amplitudes among compartments for these variables may not coincide.
Different flow patterns impact how strain and strain rate develop as compartmental volume crests to its final value. Notably, as inflation proceeds, strain rate may rise or fall even as total strain, a monotonic function of volume, steadily (and predictably) rises. Which flow pattern serves best to minimize the maximal strain rate and VILI risk experienced within any sector, therefore, may strongly depend on the nature and heterogeneity of the mechanical properties of the injured lung.
通过通气造成肺损伤(呼吸机所致肺损伤,VILI)需要反复消耗能量并产生损伤性应力。对具有均匀阻力和顺应性参数的被动充气单室肺进行数学建模表明,标准临床模式(气流模式)在能量输送的时间和强度方面存在显著差异,即决定实质应力和应变的周期内功率(ICP)。尽管弹性ICP测量值可能准确表征整体能量输送的瞬时速率,但输送到一个腔室的ICP分量如何影响与VILI相关的应变变量,取决于腔室力学、腔室大小和气体输送模式。我们将单室ICP模型扩展到了一个多室环境,该环境改变了这些特征。
该模型/模拟的主要发现表明:(1)在模拟腔室内经历的应变和应变率分别是输送能量和功率的非线性函数;(2)对于给定的气流轮廓和潮气量组合,静息腔室容积会影响其在呼吸输送时产生的最大应变;(3)气流轮廓是多室肺内最大应变以及最大应变率的关键决定因素。这意味着,临床医生选择的不同气流轮廓不仅会影响功率输送的时间,还会在具有不同力学特性的腔室之间空间分布伴随的扩张应变。重要的是,腔室ICP、应变和应变率曲线的轮廓和大小并不一致;应变和应变率不一定遵循腔室ICP,并且这些变量在腔室之间的幅度层次可能不一致。
不同的气流模式会影响应变和应变率在腔室容积达到最终值时的发展情况。值得注意的是,随着充气过程的进行,即使总应变(容积的单调函数)稳步(且可预测地)增加,应变率可能上升或下降。因此,哪种气流模式最有助于将任何区域内经历的最大应变率和VILI风险降至最低,可能很大程度上取决于受损肺的力学特性的性质和异质性。