Department of Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Vanderbilt University Institute of Imaging Science, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
J Magn Reson Imaging. 2023 Feb;57(2):598-608. doi: 10.1002/jmri.28281. Epub 2022 Jun 3.
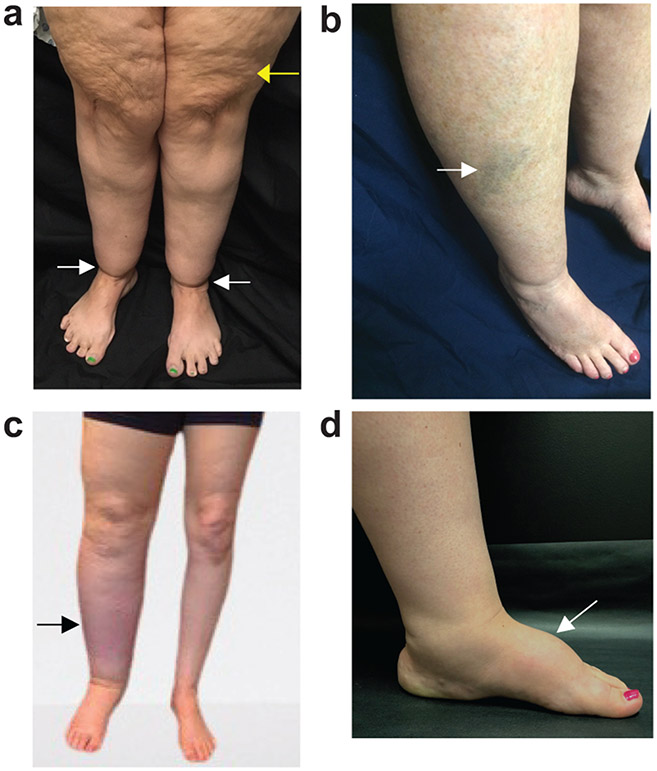
Lipedema exhibits excessive lower-extremity subcutaneous adipose tissue (SAT) deposition, which is frequently misidentified as obesity until lymphedema presents. MR lymphangiography may have relevance to distinguish lipedema from obesity or lymphedema.
Hyperintensity profiles on 3T MR lymphangiography can identify distinct features consistent with SAT edema in participants with lipedema.
Prospective cross-sectional study.
Participants (48 females, matched for age [mean = 44.8 years]) with lipedema (n = 14), lipedema with lymphedema (LWL, n = 12), cancer treatment-related lymphedema (lymphedema, n = 8), and controls without these conditions (n = 14).
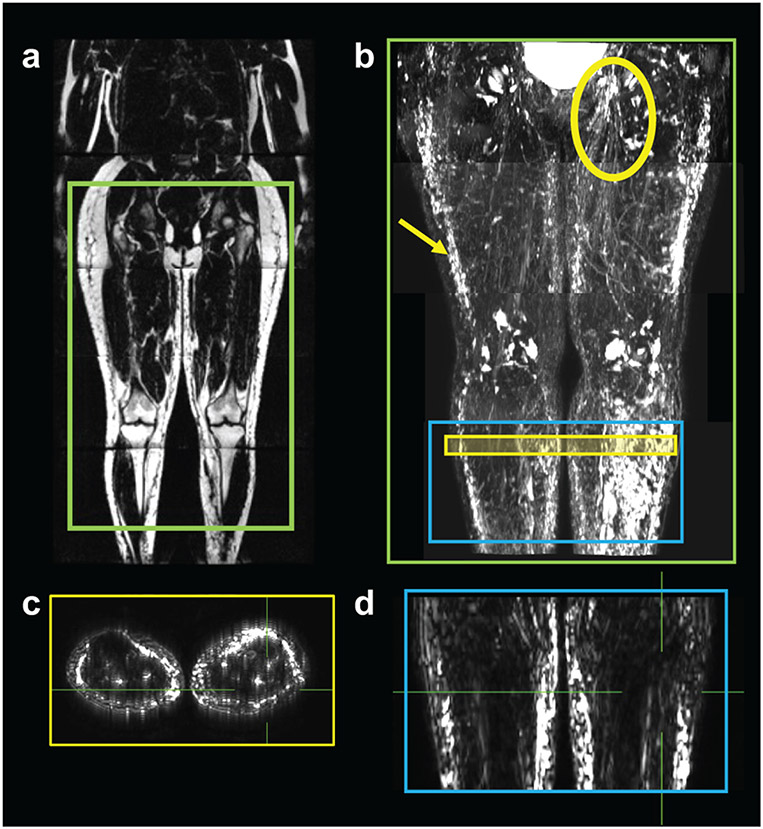
FIELD STRENGTH/SEQUENCE: 3T MR lymphangiography (nontracer 3D turbo-spin-echo).
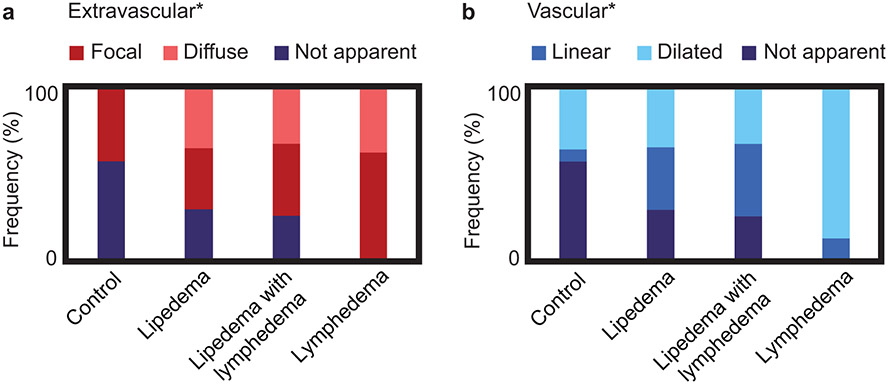
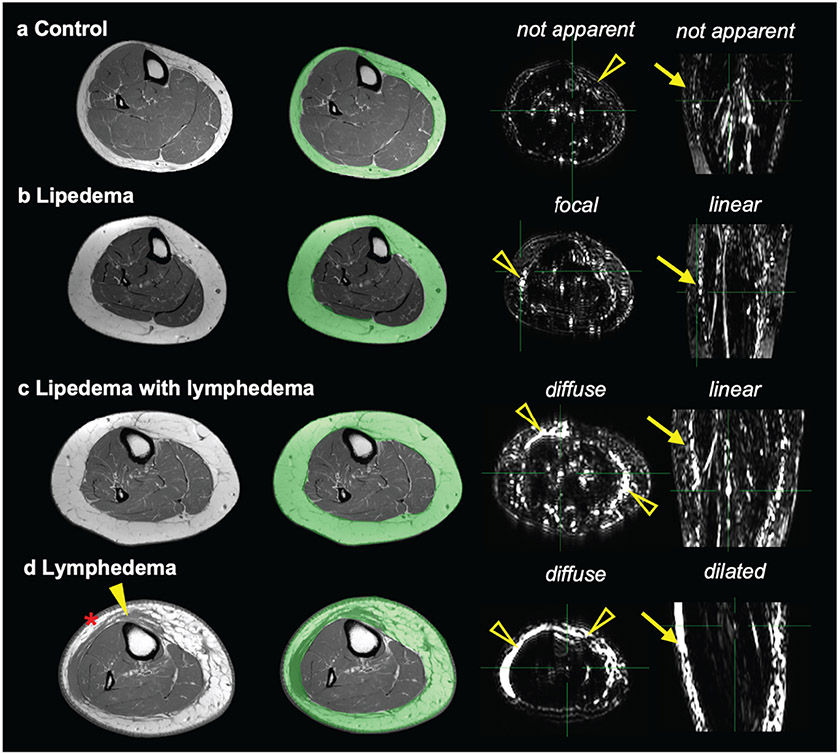
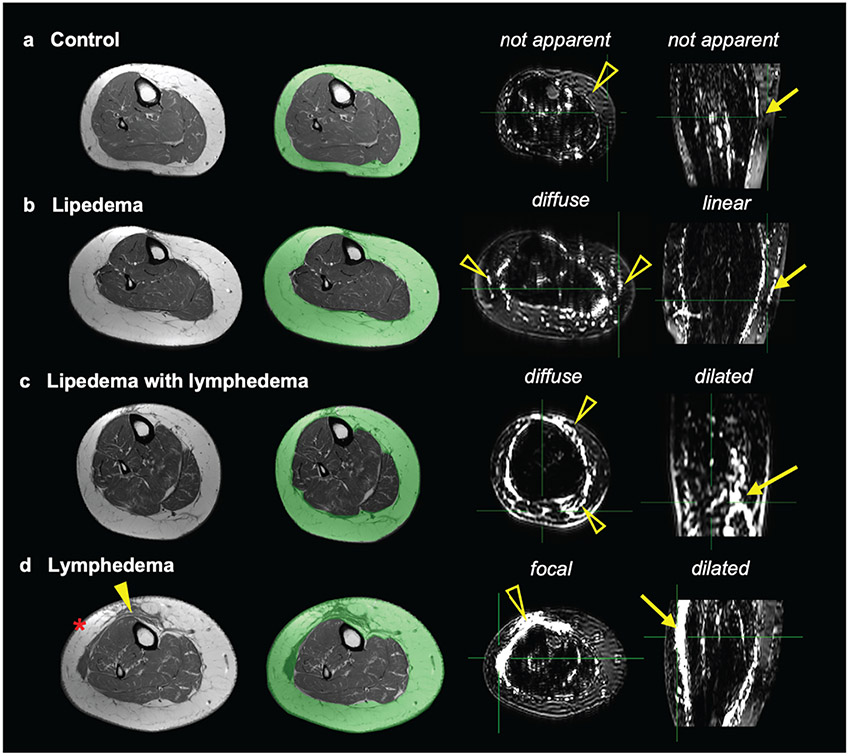
Review of lymphangiograms in lower extremities by three radiologists was performed independently. Spatial patterns of hyperintense signal within the SAT were scored for extravascular (focal, diffuse, or not apparent) and vascular (linear, dilated, or not apparent) image features.
Interreader reliability was computed using Fleiss Kappa. Fisher's exact test was used to evaluate the proportion of image features between study groups. Multinomial logistic regression was used to assess the relationship between image features and study groups. The odds ratio (OR) and 95% confidence interval (CI) of SAT extravascular and vascular features was reported in groups compared to lipedema. The threshold of statistical significance was P < 0.05.
Reliable agreement was demonstrated between three independent, blinded reviewers (P < 0.001). The frequency of SAT hyperintensities in participants with lipedema (36% focal, 36% diffuse), LWL (42% focal, 33% diffuse), lymphedema (62% focal, 38% diffuse), and controls (43% focal, 0% diffuse) was significantly distinct. Compared with lipedema, SAT hyperintensities were less frequent in controls (focal: OR = 0.63, CI = 0.11-3.41; diffuse: OR = 0.05, CI = 0.00-1.27), similar in LWL (focal: OR = 1.29, CI = 0.19-8.89; diffuse: OR = 1.05, CI = 0.15-7.61), and more frequent in lymphedema (focal: OR = 9.00, CI = 0.30-274.12; diffuse: OR = 5.73, CI = 0.18-186.84).
Noninvasive MR lymphangiography identifies distinct signal patterns indicating SAT edema and lymphatic load in participants with lipedema.
1 TECHNICAL EFFICACY: Stage 1.
脂肪水肿表现为下肢皮下脂肪组织(SAT)过度沉积,直到出现淋巴水肿才常被误认为肥胖。磁共振淋巴管造影术(MR 淋巴造影)可能有助于区分脂肪水肿与肥胖或淋巴水肿。
3T MR 淋巴造影上的高信号特征可识别出与脂肪水肿患者 SAT 水肿一致的特征。
前瞻性横断面研究。
参与者(48 名女性,年龄匹配[平均 44.8 岁]),包括脂肪水肿患者(n=14)、脂肪水肿伴淋巴水肿(LWL,n=12)、癌症治疗相关淋巴水肿(淋巴水肿,n=8)和无这些情况的对照组(n=14)。
磁场强度/序列:3T MR 淋巴造影(非示踪剂 3D 涡轮自旋回波)。
由三位放射科医生独立评估下肢淋巴造影。对 SAT 内高信号的血管外(局灶性、弥漫性或不明显)和血管(线性、扩张或不明显)图像特征进行评分。
采用 Fleiss Kappa 计算读者间可靠性。Fisher 确切检验用于评估研究组之间图像特征的比例。多变量逻辑回归用于评估图像特征与研究组之间的关系。报告了 SAT 血管外和血管特征在各研究组与脂肪水肿患者比较的比值比(OR)和 95%置信区间(CI)。统计显著性阈值为 P<0.05。
三位独立、盲法的评审员之间显示出可靠的一致性(P<0.001)。脂肪水肿患者(36%局灶性,36%弥漫性)、LWL(42%局灶性,33%弥漫性)、淋巴水肿(62%局灶性,38%弥漫性)和对照组(43%局灶性,0%弥漫性)的 SAT 高信号频率存在显著差异。与脂肪水肿相比,对照组 SAT 高信号的频率较低(局灶性:OR=0.63,CI=0.11-3.41;弥漫性:OR=0.05,CI=0.00-1.27),LWL 相似(局灶性:OR=1.29,CI=0.19-8.89;弥漫性:OR=1.05,CI=0.15-7.61),而淋巴水肿的频率较高(局灶性:OR=9.00,CI=0.30-274.12;弥漫性:OR=5.73,CI=0.18-186.84)。
非侵入性磁共振淋巴管造影术可识别出指示 SAT 水肿和脂肪水肿患者淋巴负荷的特征性信号模式。
1 技术功效:阶段 1。