Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Dutch Federation of Cancer Patient Organizations, Utrecht, The Netherlands.
BMC Prim Care. 2022 Jun 4;23(1):145. doi: 10.1186/s12875-022-01746-3.
The growing number of cancer survivors and treatment possibilities call for more personalised and integrated cancer care. Primary care seems well positioned to support this. We aimed to assess the effects of structured follow-up of a primary care team after a cancer diagnosis.
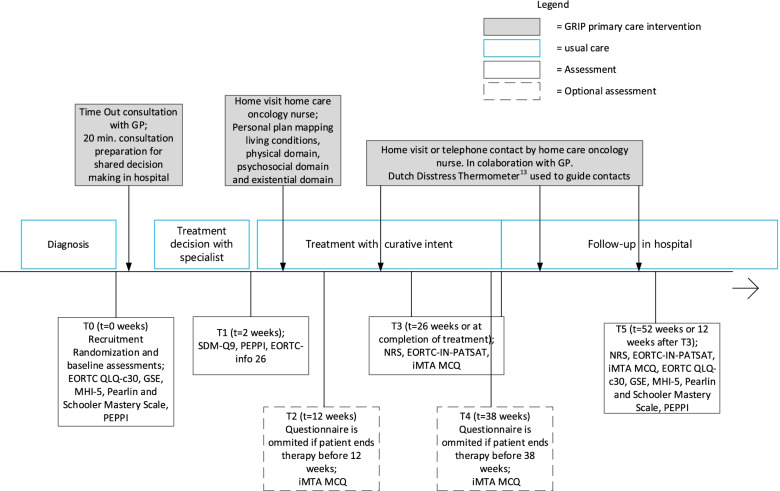
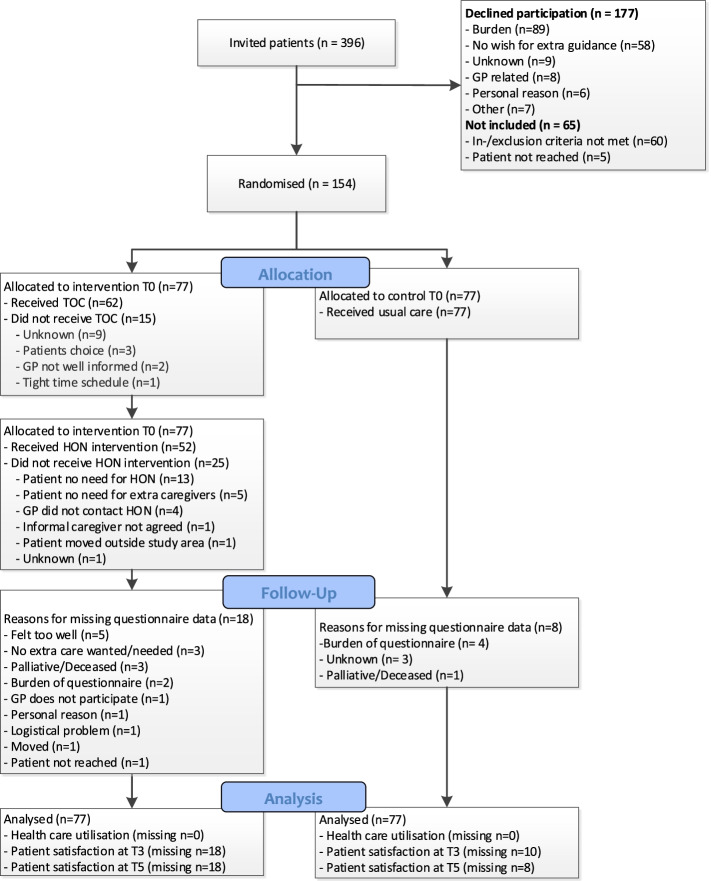
We performed a multicentre randomised controlled trial enrolling patients curatively treated for breast, lung, colorectal, gynaecologic cancer or melanoma. In addition to usual cancer care in the control group, patients randomized to intervention were offered a "Time Out consultation" (TOC) with the general practitioner (GP) after diagnosis, and subsequent follow-up during and after treatment by a home care oncology nurse (HON). Primary outcomes were patient satisfaction with care (questionnaire: EORTC-INPATSAT-32) and healthcare utilisation. Intention-to-treat linear mixed regression analyses were used for satisfaction with care and other continuous outcome variables. The difference in healthcare utilisation for categorical data was calculated with a Pearson Chi-Square or a Fisher exact test and count data (none versus any) with a log-binomial regression.
We included 154 patients (control n = 77, intervention n = 77) who were mostly female (75%), mainly diagnosed with breast cancer (51%), and had a mean age of 61 (SD ± 11.9) years. 81% of the intervention patients had a TOC and 68% had HON contact. Satisfaction with care was high (8 out of 10) in both study groups. At 3 months after treatment, GP satisfaction was significantly lower in the intervention group on 3 of 6 subscales, i.e., quality (- 14.2 (95%CI -27.0;-1.3)), availability (- 15,9 (- 29.1;-2.6)) and information provision (- 15.2 (- 29.1;-1.4)). Patients in the intervention group visited the GP practice and the emergency department more often ((RR 1.3 (1.0;1.7) and 1.70 (1.0;2.8)), respectively).
In conclusion, the GRIP intervention, which was designed to involve the primary care team during and after cancer treatment, increased the number of primary healthcare contacts. However, it did not improve patient satisfaction with care and it increased emergency department visits. As the high uptake of the intervention suggests a need of patients, future research should focus on optimizing the design and implementation of the intervention.
GRIP is retrospectively (21/06/2016) registered in the 'Netherlands Trial Register' (NTR5909).
癌症幸存者人数的增加和治疗方案的多样化要求提供更加个性化和综合的癌症护理。初级保健似乎非常适合提供这种护理。我们旨在评估在癌症诊断后由初级保健团队进行结构化随访的效果。
我们进行了一项多中心随机对照试验,纳入了接受乳腺癌、肺癌、结直肠癌、妇科癌症或黑色素瘤根治性治疗的患者。除了对照组中的常规癌症护理外,随机分配到干预组的患者在诊断后接受全科医生(GP)的“Time Out 咨询”(TOC),并在治疗期间和治疗后由家庭护理肿瘤护士(HON)进行后续随访。主要结局是患者对护理的满意度(问卷:EORTC-INPATSAT-32)和医疗保健利用情况。使用意向治疗线性混合回归分析评估护理满意度和其他连续结局变量。使用 Pearson Chi-Square 或 Fisher 精确检验计算分类数据的医疗保健利用差异,使用对数二项式回归计算无与有(无与任何)的计数数据。
我们纳入了 154 名患者(对照组 n=77,干预组 n=77),他们主要是女性(75%),主要诊断为乳腺癌(51%),平均年龄为 61 岁(标准差±11.9)。81%的干预患者接受了 TOC,68%的患者接受了 HON 接触。两组患者对护理的满意度均较高(均为 8 分)。治疗后 3 个月,干预组在 6 个亚量表中的 3 个上,即质量(-14.2(95%CI-27.0;-1.3))、可用性(-15,9(-29.1;-2.6))和信息提供(-15.2(-29.1;-1.4))方面,GP 满意度明显较低。干预组患者更频繁地就诊于全科医生诊所和急诊(分别为(RR 1.3(1.0;1.7)和 1.70(1.0;2.8)))。
总之,GRIP 干预旨在在癌症治疗期间和之后让初级保健团队参与其中,增加了初级保健的接触次数。然而,它并没有提高患者对护理的满意度,反而增加了急诊就诊次数。由于干预措施的高接受率表明患者有需求,因此未来的研究应侧重于优化干预措施的设计和实施。
GRIP 是在(2016 年 6 月 21 日)回顾性注册于“荷兰试验注册库”(NTR5909)。