Usher Institute, University of Edinburgh, Edinburgh, UK.
School of Health in Social Science, University of Edinburgh, Edinburgh, UK.
Int J Obes (Lond). 2022 Sep;46(9):1624-1632. doi: 10.1038/s41366-022-01157-5. Epub 2022 Jun 3.
To analyse the Growing Up in Scotland cohort for predictors of obesity at age 12, present at school entry (age 5-6).
The initial model included literature-based risk factors likely to be routinely collected in high-income countries (HICs), as well as "Adverse/Protective Childhood Experiences (ACEs/PCEs)". Missing data were handled by Multiple Chained Equations. Variable-reduction was performed using multivariable logistic regression with backwards and forwards stepwise elimination, followed by internal validation by bootstrapping. Optimal sensitivity/specificity cut-offs for the most parsimonious and accurate models in two situations (optimum available data, and routinely available data in Scotland) were examined for their referral burden, and Positive and Negative Predictive Values.
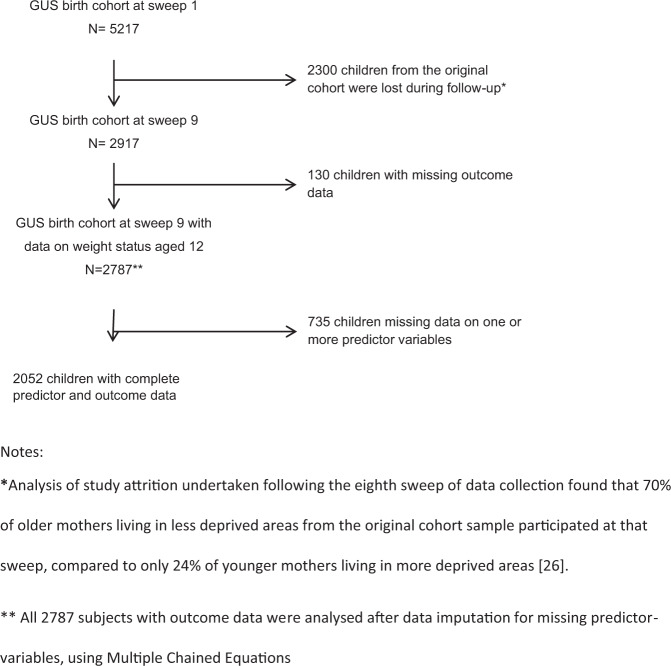
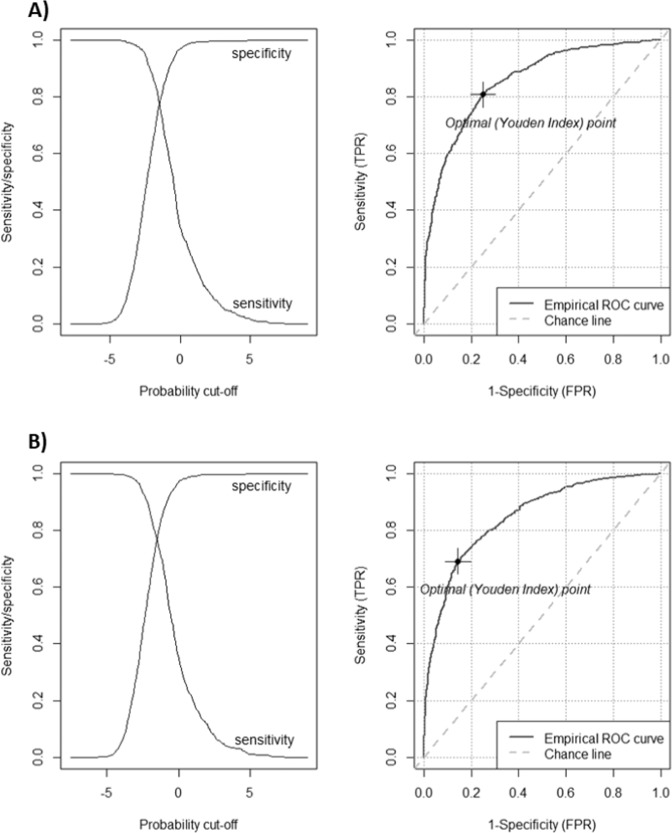
Data for 2787 children with full outcome data (obesity prevalence 18.3% at age 12) were used to develop the models. The final "Optimum Data" model included six predictors of obesity: maternal body mass index, indoor smoking, equivalized income quintile, child's sex, child's BMI at age 5-6, and ACEs. After internal validation, the area under the receiver operating characteristic curve was 0.855 (95% CI 0.852-0.859). A cut-off based on Youden's J statistic for the Optimum Data model yielded a specificity of 77.6% and sensitivity of 76.3%. 37.0% of screened children were "Total Screen Positives" (and thus would constitute the "referral burden".) A "Scottish Data" model, without equivalized income quintile and ACEs as a predictor, and instead using Scottish Index of Multiple Deprivation quintile and "age at introduction of solid foods," was slightly less sensitive (76.2%) but slightly more specific (79.2%), leading to a smaller referral burden (30.8%).
Universally collected, machine readable and linkable data at age 5-6 predict reasonably well children who will be obese by age 12. However, the Scottish treatment system is unable to cope with the resultant referral burden and other criteria for screening would have to be met.
分析苏格兰成长队列中 12 岁时肥胖的预测因素,这些因素在入学时(5-6 岁)就存在。
初始模型包括基于文献的、可能在高收入国家(HICs)常规收集的风险因素,以及“不良/保护性儿童经历(ACEs/PCEs)”。缺失数据通过多重链式方程处理。使用向后和向前逐步消除的多变量逻辑回归进行变量缩减,然后通过自举进行内部验证。对于两种情况(最佳可用数据和苏格兰常规可用数据)最简洁和准确的模型,检查最佳灵敏度/特异性截断值的转诊负担,以及阳性和阴性预测值。
使用 2787 名具有完整结局数据的儿童(12 岁时肥胖患病率为 18.3%)数据来建立模型。最终的“最佳数据”模型包括肥胖的六个预测因素:母亲的体重指数、室内吸烟、等效收入五分位数、儿童的性别、儿童 5-6 岁时的 BMI 和 ACEs。内部验证后,接收者操作特征曲线下的面积为 0.855(95%CI 0.852-0.859)。基于 Youden 的 J 统计量的最佳数据模型截断值产生了 77.6%的特异性和 76.3%的敏感性。37.0%的筛查儿童为“总筛查阳性”(因此构成“转诊负担”)。没有等效收入五分位数和 ACEs 作为预测因素的“苏格兰数据”模型,而是使用苏格兰多重剥夺五分位数和“固体食物引入年龄”,敏感性略低(76.2%),但特异性略高(79.2%),导致转诊负担较小(30.8%)。
在 5-6 岁时普遍收集的、机器可读的和可链接的数据可以很好地预测到 12 岁时肥胖的儿童。然而,苏格兰的治疗系统无法应对由此产生的转诊负担,必须满足其他筛选标准。