Department of Pediatrics, University Hospitals Leuven, Leuven, Belgium.
KU Leuven Department of Microbiology, Immunology and Transplantation, Rega Institute, Laboratory of Clinical and Epidemiological Virology, Leuven, Belgium.
PLoS One. 2022 Jun 6;17(6):e0268532. doi: 10.1371/journal.pone.0268532. eCollection 2022.
We aimed to provide regional data on clinical symptoms, medical resource utilization (MRU), and risk factors for increased MRU in hospitalized respiratory syncytial virus (RSV)-infected Belgian pediatric population.
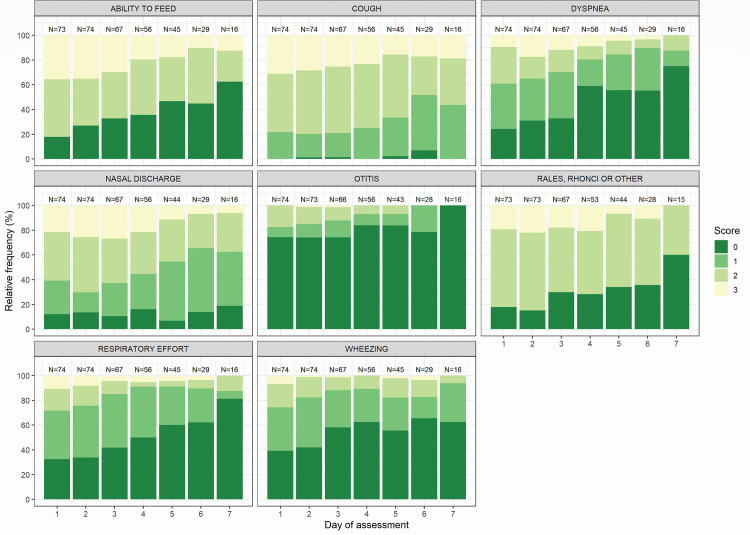
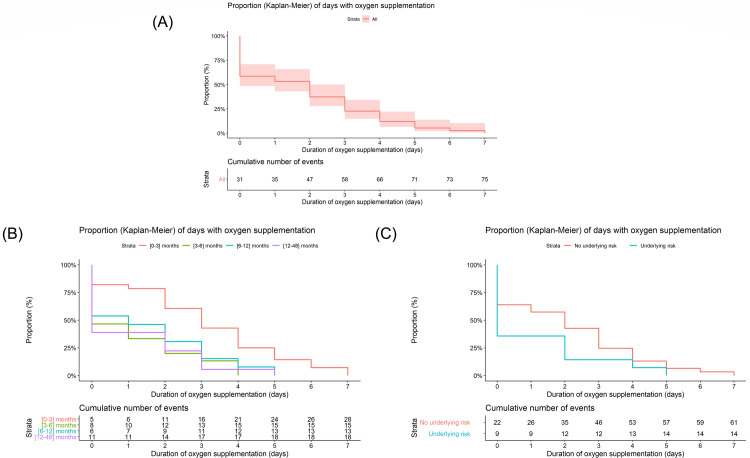
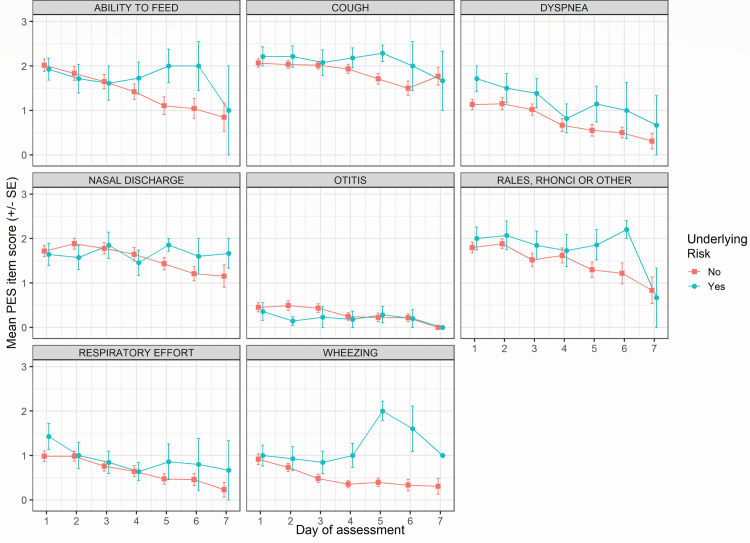
This prospective, multicenter study enrolled RSV (+) hospitalized children (aged ≤5y) during the 2013-2015 RSV seasons. RSV was diagnosed within 24h of hospitalization. Disease severity of RSV (+) patients was assessed until discharge or up to maximum six days using a Physical Examination Score (PES) and a derived score based on ability to feed, dyspnea and respiratory effort (PES3). MRU (concomitant medications, length of hospitalization [LOH], and oxygen supplementation) was evaluated. Kaplan-Meier survival analysis was performed to compare MRU by age and presence of risk factors for severe disease. Association between baseline covariates and MRU was analyzed using Cox regression models.
In total, 75 children were included, Median (range) age was 4 (0-41) months, risk factors were present in 18.7%, and early hospitalization (≤3 days of symptom onset) was observed in 57.3% of patients. Cough (100%), feeding problems (82.2%), nasal discharge (87.8%), and rales and rhonchi (82.2%) were frequently observed. Median (range) LOH and oxygen supplementation was 5 (2-7) and 3 (1-7) days. Oxygen supplementation, bronchodilators, and antibiotics were administered to 58.7%, 64.0%, and 41.3% of the patients, respectively. Age <3 months and baseline total PES3 score were associated with probability and the duration of receiving oxygen supplementation. LOH was not associated with any covariate.
RSV is associated with high disease burden and MRU in hospitalized children. Oxygen supplementation but not length of hospitalization was associated with very young age and the PES3 score. These results warrant further assessment of the PES3 score as a predictor for the probability of receiving and length of oxygen supplementation in RSV hospitalized children.
NCT02133092.
本研究旨在提供比利时儿科住院呼吸道合胞病毒(RSV)感染患者的临床症状、医疗资源利用(MRU)和增加 MRU 风险因素的区域数据。
这是一项前瞻性、多中心研究,纳入了 2013-2015 年 RSV 季节期间住院的 RSV(+)感染的≤5 岁儿童。RSV 是在住院后 24 小时内确诊的。采用体格检查评分(PES)和基于喂养能力、呼吸困难和呼吸努力的衍生评分(PES3)对 RSV(+)患者的疾病严重程度进行评估,直至出院或最长 6 天。评估了 MRU(同时使用的药物、住院时间[LOH]和氧疗)。采用 Kaplan-Meier 生存分析比较不同年龄和严重疾病风险因素患者的 MRU。采用 Cox 回归模型分析基线协变量与 MRU 的关系。
共纳入 75 例患儿,中位(范围)年龄为 4(0-41)个月,有危险因素的占 18.7%,57.3%的患儿为早期住院(症状发作后≤3 天)。咳嗽(100%)、喂养问题(82.2%)、鼻分泌物(87.8%)和啰音及喘鸣(82.2%)较为常见。中位(范围)LOH 和氧疗时间分别为 5(2-7)和 3(1-7)天。58.7%、64.0%和 41.3%的患儿分别接受了氧疗、支气管扩张剂和抗生素治疗。年龄<3 个月和基线总 PES3 评分与氧疗的概率和持续时间相关。LOH 与任何协变量均无关。
RSV 导致住院患儿疾病负担高且医疗资源利用率高。氧疗而非住院时间与年龄较小和 PES3 评分有关。这些结果表明,需要进一步评估 PES3 评分作为预测 RSV 住院患儿接受氧疗的概率和时间的指标。
NCT02133092。