Lab for Research on Ethics, Aging and Community Health, Departments of Occupational Therapy and Community Health, Tufts University, Medford, Massachusetts.
William B. Schwartz MD Division of Nephrology, Tufts Medical Center, Boston, Massachusetts.
Clin J Am Soc Nephrol. 2022 Jul;17(7):957-965. doi: 10.2215/CJN.13241021. Epub 2022 Jun 7.
Coronavirus disease 2019 (COVID-19) disrupted medical care across health care settings for older patients with advanced CKD. Understanding how shared decision making for kidney treatment decisions was influenced by the uncertainty of an evolving pandemic can provide insights for supporting shared decision making through the current and future public health crises.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We performed thematic and narrative analyses of semistructured interviews with patients (CKD stages 4 and 5, age 70+), care partners, and clinicians from Boston, Portland (Maine), San Diego, and Chicago from August to December 2020.
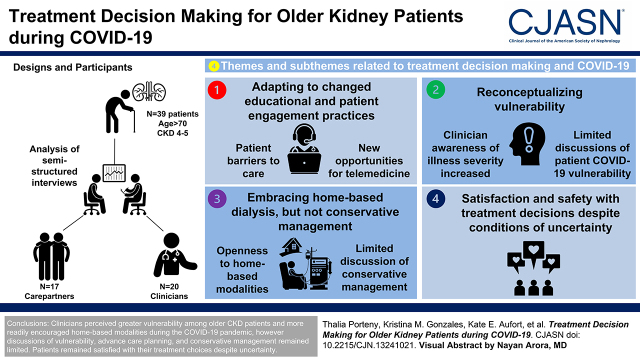
We interviewed 76 participants (39 patients, 17 care partners, and 20 clinicians). Among patient participants, 13 (33%) patients identified as Black, and seven (18%) had initiated dialysis. Four themes with corresponding subthemes emerged related to treatment decision making and the COVID-19 pandemic: () adapting to changed educational and patient engagement practices (patient barriers to care and new opportunities for telemedicine); () reconceptualizing vulnerability (clinician awareness of illness severity increased and limited discussions of patient COVID-19 vulnerability); () embracing home-based dialysis but not conservative management (openness to home-based modalities and limited discussion of conservative management and advanced care planning); and () satisfaction and safety with treatment decisions despite conditions of uncertainty.
Although clinicians perceived greater vulnerability among older patients CKD and more readily encouraged home-based modalities during the COVID-19 pandemic, their discussions of vulnerability, advance care planning, and conservative management remained limited, suggesting areas for improvement. Clinicians reported burnout caused by the pandemic, increased time demands, and workforce limitations, whereas patients remained satisfied with their treatment choices despite uncertainty.
Decision Aid for Renal Therapy (DART), NCT03522740.
2019 年冠状病毒病(COVID-19)在整个医疗保健环境中扰乱了老年晚期慢性肾脏病(CKD)患者的医疗服务。了解治疗决策的共同决策如何受到不断演变的大流行的不确定性的影响,可以为通过当前和未来的公共卫生危机支持共同决策提供见解。
设计、地点、参与者和测量:我们对来自波士顿、波特兰(缅因州)、圣地亚哥和芝加哥的 2020 年 8 月至 12 月的患者(CKD 4 期和 5 期,年龄 70 岁以上)、护理伙伴和临床医生进行了半结构化访谈的主题和叙述分析。
我们采访了 76 名参与者(39 名患者、17 名护理伙伴和 20 名临床医生)。在患者参与者中,13 名(33%)患者为黑人,7 名(18%)已开始透析。有四个主题和相应的子主题与治疗决策和 COVID-19 大流行有关:(1)适应教育和患者参与实践的变化(患者就医障碍和远程医疗的新机会);(2)重新概念化脆弱性(临床医生对疾病严重程度的认识提高,对患者 COVID-19 脆弱性的讨论有限);(3)接受家庭为基础的透析,但不接受保守管理(对家庭为基础的模式开放,对保守管理和先进的护理计划的讨论有限);(4)尽管存在不确定性,但对治疗决策感到满意和安全。
尽管临床医生认为老年 CKD 患者的脆弱性更大,并在 COVID-19 大流行期间更积极地鼓励家庭为基础的模式,但他们对脆弱性、预先护理计划和保守管理的讨论仍然有限,这表明需要改进的地方。临床医生报告说,大流行导致倦怠、时间需求增加和劳动力限制,而患者尽管存在不确定性,但仍对他们的治疗选择感到满意。
肾脏治疗决策辅助工具(DART),NCT03522740。