O'Donnell Martin J, McQueen Matthew, Sniderman Allan, Pare Guillaume, Wang Xingyu, Hankey Graeme J, Rangarajan Sumathy, Chin Siu Lim, Rao-Melacini Purnima, Ferguson John, Xavier Denis, Lisheng Liu, Zhang Hongye, Pais Prem, Lopez-Jaramillo Patricio, Damasceno Albertino, Langhorne Peter, Rosengren Annika, Dans Antonio L, Elsayed Ahmed, Avezum Alvaro, Mondo Charles, Judge Conor, Diener Hans-Christoph, Ryglewicz Danuta, Czlonkowska Anna, Pogosova Nana, Weimar Christian, Iqbal Romana, Diaz Rafael, Yusoff Khalid, Yusufali Afzalhussein, Oguz Aytekin, Penaherrera Ernesto, Lanas Fernando, Ogah Okechukwu S, Ogunniyi Adesola, Iversen Helle K, Malaga German, Rumboldt Zvonko, Oveisgharan Shahram, Al Hussain Fawaz, Nilanont Yongchai, Yusuf Salim
Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, ON, Canada.
Department of Medicine, HRB-Clinical Research Facility, NUI Galway, Galway, Ireland.
J Stroke. 2022 May;24(2):224-235. doi: 10.5853/jos.2021.02152. Epub 2022 May 31.
The association of dyslipidemia with stroke has been inconsistent, which may be due to differing associations within etiological stroke subtypes. We sought to determine the association of lipoproteins and apolipoproteins within stroke subtypes.
Standardized incident case-control STROKE study in 32 countries. Cases were patients with acute hospitalized first stroke, and matched by age, sex and site to controls. Concentrations of total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (apoA1), and apoB were measured. Non-HDL-C was calculated. We estimated multivariable odds ratio (OR) and population attributable risk percentage (PAR%). Outcome measures were all stroke, ischemic stroke (and subtypes), and intracerebral hemorrhage (ICH).
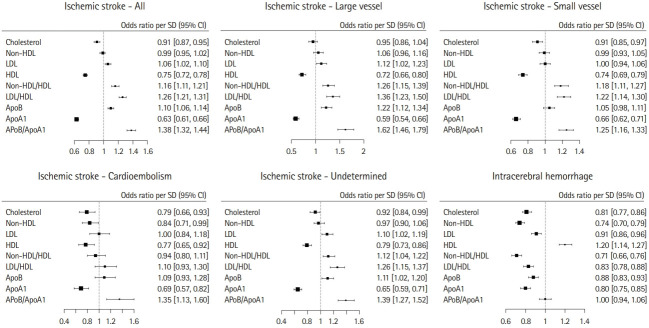
Our analysis included 11,898 matched case-control pairs; 77.3% with ischemic stroke and 22.7% with ICH. Increasing apoB (OR, 1.10; 95% confidence interval [CI], 1.06 to 1.14 per standard deviation [SD]) and LDL-C (OR, 1.06; 95% CI, 1.02 to 1.10 per SD) were associated with an increase in risk of ischemic stroke, but a reduced risk of ICH. Increased apoB was significantly associated with large vessel stroke (PAR 13.4%; 95% CI, 5.6 to 28.4) and stroke of undetermined cause. Higher HDL-C (OR, 0.75; 95% CI, 0.72 to 0.78 per SD) and apoA1 (OR, 0.63; 95% CI, 0.61 to 0.66 per SD) were associated with ischemic stroke (and subtypes). While increasing HDL-C was associated with an increased risk of ICH (OR, 1.20; 95% CI, 1.14 to 1.27 per SD), apoA1 was associated with a reduced risk (OR, 0.80; 95% CI, 0.75 to 0.85 per SD). ApoB/A1 (OR, 1.38; 95% CI, 1.32 to 1.44 per SD) had a stronger magnitude of association than the ratio of LDL-C/HDL-C (OR, 1.26; 95% CI, 1.21 to 1.31 per SD) with ischemic stroke (P<0.0001).
The pattern and magnitude of association of lipoproteins and apolipoproteins with stroke varies by etiological stroke subtype. While the directions of association for LDL, HDL, and apoB were opposing for ischemic stroke and ICH, apoA1 was associated with a reduction in both ischemic stroke and ICH. The ratio of apoB/A1 was the best lipid predictor of ischemic stroke risk.
血脂异常与中风之间的关联并不一致,这可能是由于病因性中风亚型之间的关联不同。我们试图确定中风亚型中脂蛋白和载脂蛋白的关联。
在32个国家进行标准化的新发病例对照中风研究。病例为首次急性住院中风患者,并按年龄、性别和部位与对照进行匹配。测量总胆固醇、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)、载脂蛋白A1(apoA1)和apoB的浓度。计算非HDL-C。我们估计多变量比值比(OR)和人群归因风险百分比(PAR%)。结局指标为所有中风、缺血性中风(及其亚型)和脑出血(ICH)。
我们的分析纳入了11,898对匹配的病例对照;77.3%为缺血性中风,22.7%为ICH。apoB升高(OR,1.10;95%置信区间[CI],每标准差[SD]为1.06至1.14)和LDL-C升高(OR,1.06;95%CI,每SD为1.02至1.10)与缺血性中风风险增加相关,但与ICH风险降低相关。apoB升高与大动脉中风(PAR 13.4%;95%CI,5.6至28.4)和病因不明的中风显著相关。较高的HDL-C(OR,0.75;95%CI,每SD为0.72至0.78)和apoA1(OR,0.63;95%CI,每SD为0.61至0.66)与缺血性中风(及其亚型)相关。虽然HDL-C升高与ICH风险增加相关(OR,1.20;95%CI,每SD为1.14至1.27),但apoA1与风险降低相关(OR,0.80;95%CI,每SD为0.75至0.85)。apoB/A1(OR,1.38;95%CI,每SD为1.32至1.44)与缺血性中风的关联强度比LDL-C/HDL-C比值(OR,1.26;95%CI,每SD为1.21至1.31)更强(P<0.0001)。
脂蛋白和载脂蛋白与中风的关联模式和强度因病因性中风亚型而异。虽然LDL、HDL和apoB与缺血性中风和ICH的关联方向相反,但apoA1与缺血性中风和ICH的风险降低均相关。apoB/A1比值是缺血性中风风险的最佳血脂预测指标。