Department of Anaesthesiology and Intensive Care, Faculty of Medical Sciences in Katowice, Medical University of Silesia, 40-752 Katowice, Poland.
Students' Scientific Society, Department of Anaesthesiology and Intensive Care, Faculty of Medical Sciences in Katowice, Medical University of Silesia, 40-752 Katowice, Poland.
Int J Environ Res Public Health. 2022 May 29;19(11):6626. doi: 10.3390/ijerph19116626.
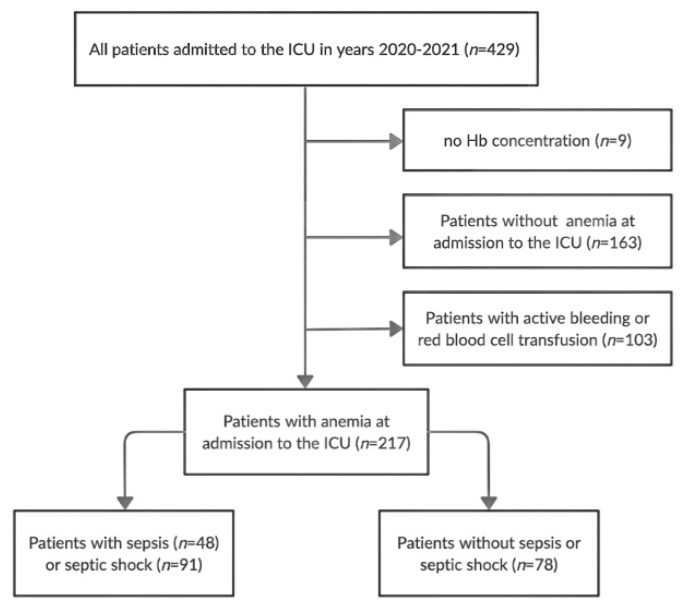
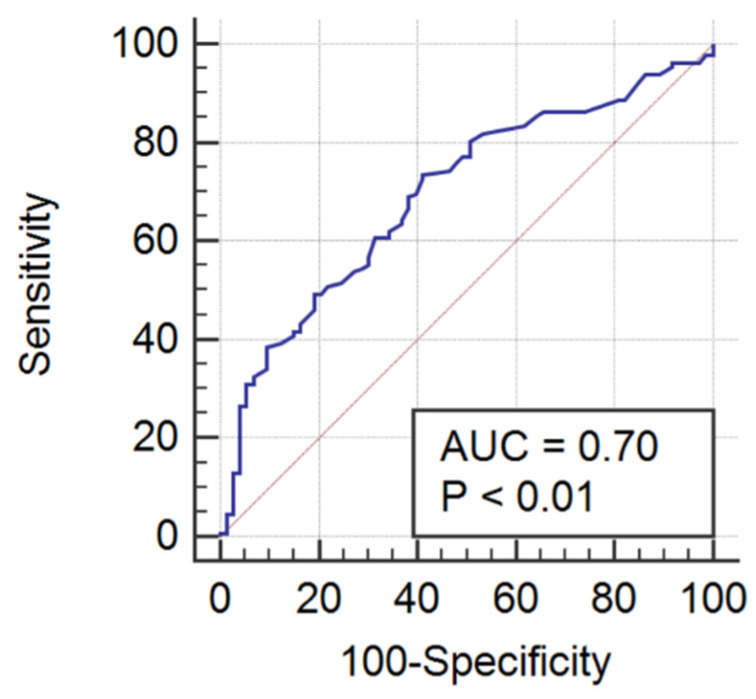
Sepsis can affect various organs as well as the hematologic system. Systemic dysregulation, present in sepsis, affects particularly red blood cells (RBCs). One of the widely available RBC indices is RBC distribution width (RDW). Sepsis may also affect hemostasis, with septic patients presenting with coagulopathy or disseminated intravascular coagulation. The aim of our study was to analyze the impact of sepsis on RBC indices and coagulation parameters on admission to the intensive care unit (ICU) and their association with presence of sepsis and sepsis outcomes in anemic critically ill patients. We performed a retrospective observational study covering consecutive patients admitted to a 10-bed mixed ICU in the years 2020−2021. We found significant differences between septic and non-septic patients for the following parameters: RDW (p = 0.02), INR (p < 0.01), aPTT (p < 0.01), D-dimers (p < 0.01), fibrinogen (p = 0.02), platelets (p = 0.04). International normalized ratio was the only parameter with adequate sepsis predictive value (AUROC = 0.70; 95% CI 0.63−0.76; p < 0.01), with an optimal cut-off value of >1.21. Combination of INR with fibrinogen and a severity of disease score improved INR’s predictive value (AUROC 0.74−0.77). Combination of INR with a severity of disease score was an adequate ICU mortality predictor in septic patients (AUROC 0.70−0.75). Sepsis significantly affects RDW and most coagulation parameters. Increased INR can be used for sepsis screening, whereas combination of INR with a severity of disease score can be a predictor of short-term mortality in septic patients.
败血症可影响多个器官和血液系统。败血症中的全身失调特别影响红细胞(RBC)。RBC 分布宽度(RDW)是广泛可用的 RBC 指标之一。败血症也可能影响止血,败血症患者表现出凝血功能障碍或弥漫性血管内凝血。我们的研究目的是分析败血症对入院时 ICU 中 RBC 指数和凝血参数的影响,以及它们与贫血危重症患者败血症和败血症结局的相关性。我们进行了一项回顾性观察研究,涵盖了 2020-2021 年入住 10 张混合 ICU 的连续患者。我们发现败血症和非败血症患者在以下参数方面存在显著差异:RDW(p=0.02)、INR(p<0.01)、aPTT(p<0.01)、D-二聚体(p<0.01)、纤维蛋白原(p=0.02)、血小板(p=0.04)。INR 是唯一具有足够败血症预测价值的参数(AUROC=0.70;95%CI 0.63-0.76;p<0.01),最佳截断值为>1.21。INR 与纤维蛋白原和疾病严重程度评分的组合提高了 INR 的预测价值(AUROC 0.74-0.77)。INR 与疾病严重程度评分的组合是败血症患者 ICU 死亡率的合适预测因子(AUROC 0.70-0.75)。败血症显著影响 RDW 和大多数凝血参数。INR 升高可用于败血症筛查,而 INR 与疾病严重程度评分的组合可预测败血症患者的短期死亡率。