Department of Cardiology, Angiology, Haemostaseology and Medical Intensive Care, 36642University Medical Centre Mannheim, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany.
European Center for AngioScience (ECAS) and German Center for Cardiovascular Research (DZHK) partner site Heidelberg/Mannheim, Mannheim, Germany.
Clin Appl Thromb Hemost. 2022 Jan-Dec;28:10760296221137893. doi: 10.1177/10760296221137893.
The study investigates the diagnostic and prognostic significance of the prothrombin time/international normalized ratio (PT/INR) in patients with sepsis and septic shock.
Sepsis may be complicated by disseminated intravascular coagulation (DIC). While the status of coagulopathy of septic patients is represented within the sepsis-3 definition by assessing the platelet count, less data regarding the prognostic impact of the PT/INR in patients admitted with sepsis and septic shock is available.
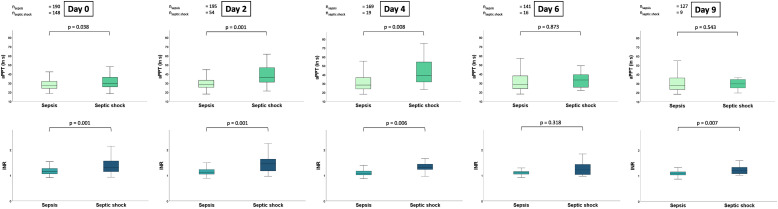
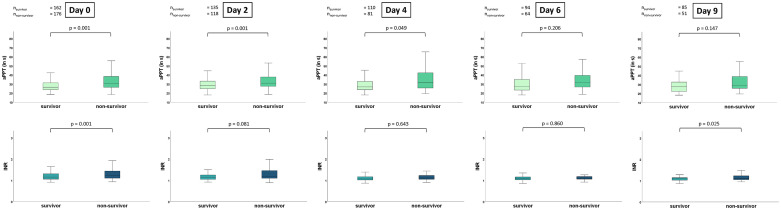
Consecutive patients with sepsis and septic shock from 2019 to 2021 were included. Blood samples were retrieved from day of disease onset (ie, day 0), as well as on day 1, 2, 4, 6 and 9 thereafter. Firstly, the diagnostic value of the PT/INR in comparison to the activated partial thromboplastin time (aPTT) was tested for septic shock compared to sepsis without shock. Secondly, the prognostic value of the PT/INR for 30-day all-cause mortality was tested. Statistical analyses included univariable t-tests, Spearman's correlations, C-statistics, Kaplan-Meier analyses and Cox proportional regression analyses.
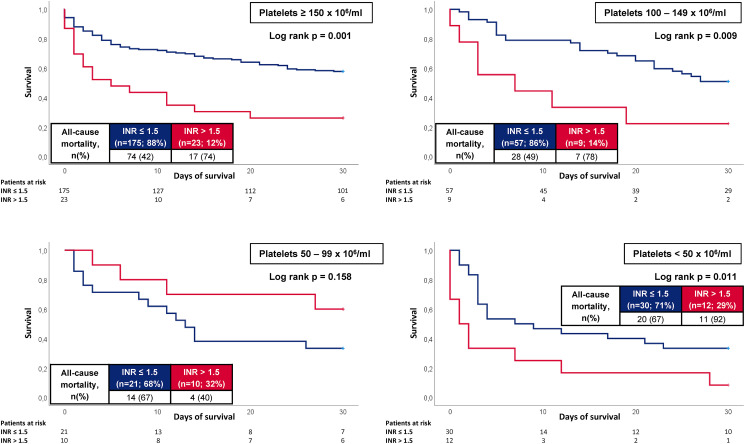
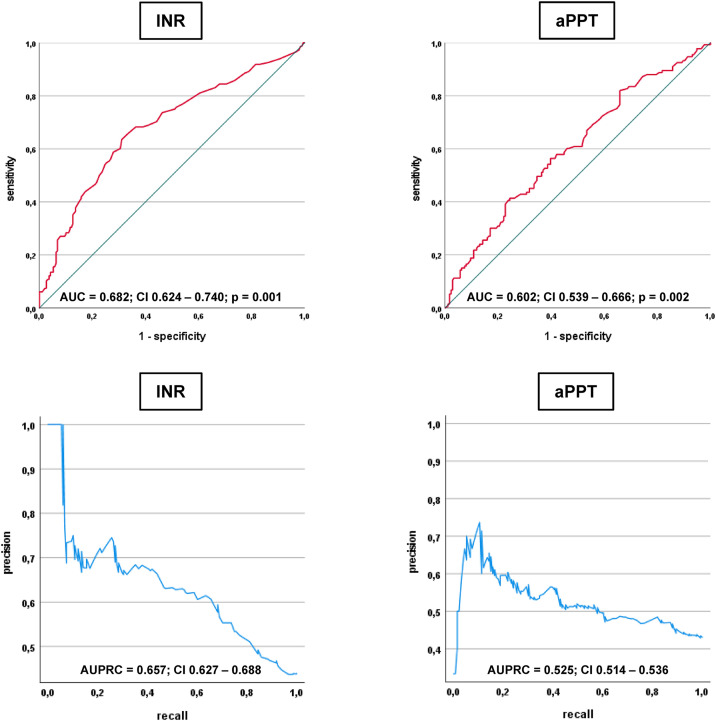
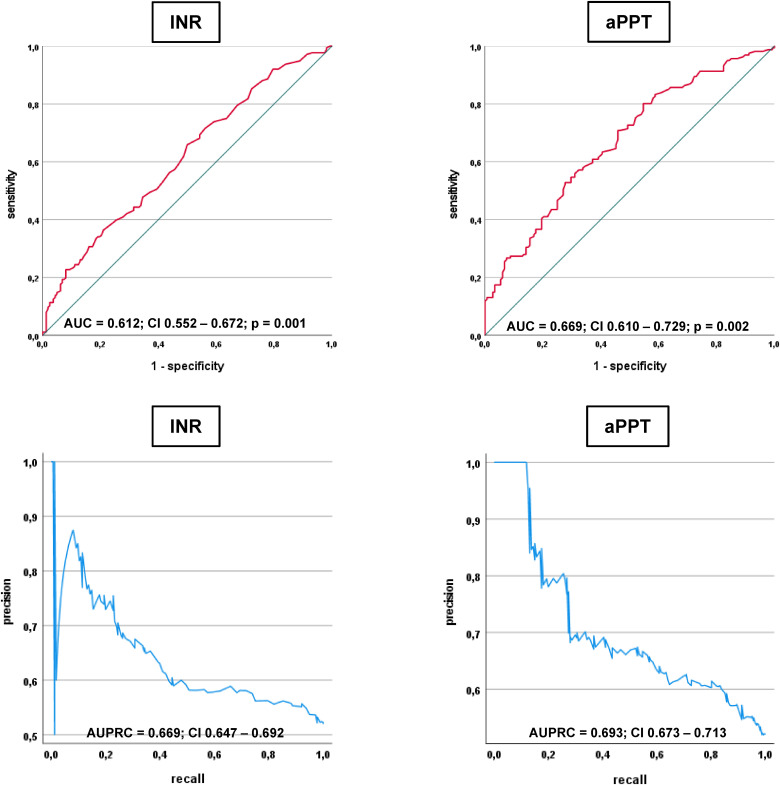
338 patients were included (56% sepsis without shock, 44% septic shock). The overall rate of all-cause mortality at 30 days was 52%. With an area under the curve (AUC) of 0.682 (= .001) on day 0, the PT/INR revealed moderate discrimination of septic shock and sepsis without shock. Furthermore, PT/ INR was able to discriminate non-survivors and survivors at 30 days (AUC = 0.612; = .001). Patients with a PT/INR >1.5 had higher rates of 30-day all-cause mortality than patients with lower values (mortality rate 73% vs 48%; log rank = .001; HR = 2.129; 95% CI 1.494-3.033; = .001), even after multivariable adjustment (HR = 1.793; 95% CI 1.343-2.392; = .001). Increased risk of 30-day all-cause mortality was observed irrespective of concomitant thrombocytopenia.
The PT/INR revealed moderate diagnostic accuracy for septic shock but was associated with reliable prognostic accuracy with regard to 30-day all-cause mortality in patients admitted with sepsis and septic shock.
本研究旨在探讨凝血酶原时间/国际标准化比值(PT/INR)在脓毒症和感染性休克患者中的诊断和预后意义。
脓毒症可能并发弥漫性血管内凝血(DIC)。虽然脓毒症-3 定义通过评估血小板计数来反映脓毒症患者凝血障碍的状态,但关于 PT/INR 在脓毒症和感染性休克患者入院时的预后影响的数据较少。
纳入了 2019 年至 2021 年期间连续的脓毒症和感染性休克患者。采集发病当天(即第 0 天)以及第 1、2、4、6 和 9 天的血样。首先,比较 PT/INR 与活化部分凝血活酶时间(aPTT)在诊断感染性休克与无休克性脓毒症方面的诊断价值。其次,测试 PT/INR 对 30 天全因死亡率的预后价值。统计分析包括单变量 t 检验、Spearman 相关性、C 统计量、Kaplan-Meier 分析和 Cox 比例风险回归分析。
共纳入 338 例患者(56%为无休克性脓毒症,44%为感染性休克)。30 天全因死亡率为 52%。在第 0 天,曲线下面积(AUC)为 0.682(=0.001),PT/INR 对感染性休克和无休克性脓毒症具有中等程度的鉴别能力。此外,PT/INR 还能够在 30 天区分存活者和非存活者(AUC=0.612;=0.001)。PT/INR>1.5 的患者 30 天全因死亡率高于 PT/INR 值较低的患者(死亡率分别为 73%和 48%;log rank=0.001;HR=2.129;95%CI 1.494-3.033;=0.001),即使在多变量调整后也是如此(HR=1.793;95%CI 1.343-2.392;=0.001)。观察到 30 天全因死亡率增加与同时存在血小板减少无关。
PT/INR 对感染性休克具有中等诊断准确性,并且与脓毒症和感染性休克患者 30 天全因死亡率相关,具有可靠的预后准确性。