Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Genitourinary Oncology, Barts Cancer Institute, Cancer Research UK Experimental Cancer Medicine Centre, Queen Mary University of London, Royal Free National Health Service Trust, London, UK.
Lancet Oncol. 2022 Jul;23(7):888-898. doi: 10.1016/S1470-2045(22)00290-X. Epub 2022 Jun 7.
In the primary analysis of CheckMate 9ER, nivolumab plus cabozantinib showed superior progression-free survival, overall survival, and objective response over sunitinib in patients with previously untreated advanced renal cell carcinoma (median follow-up of 18·1 months). Here, we report extended follow-up of overall survival and updated efficacy and safety.
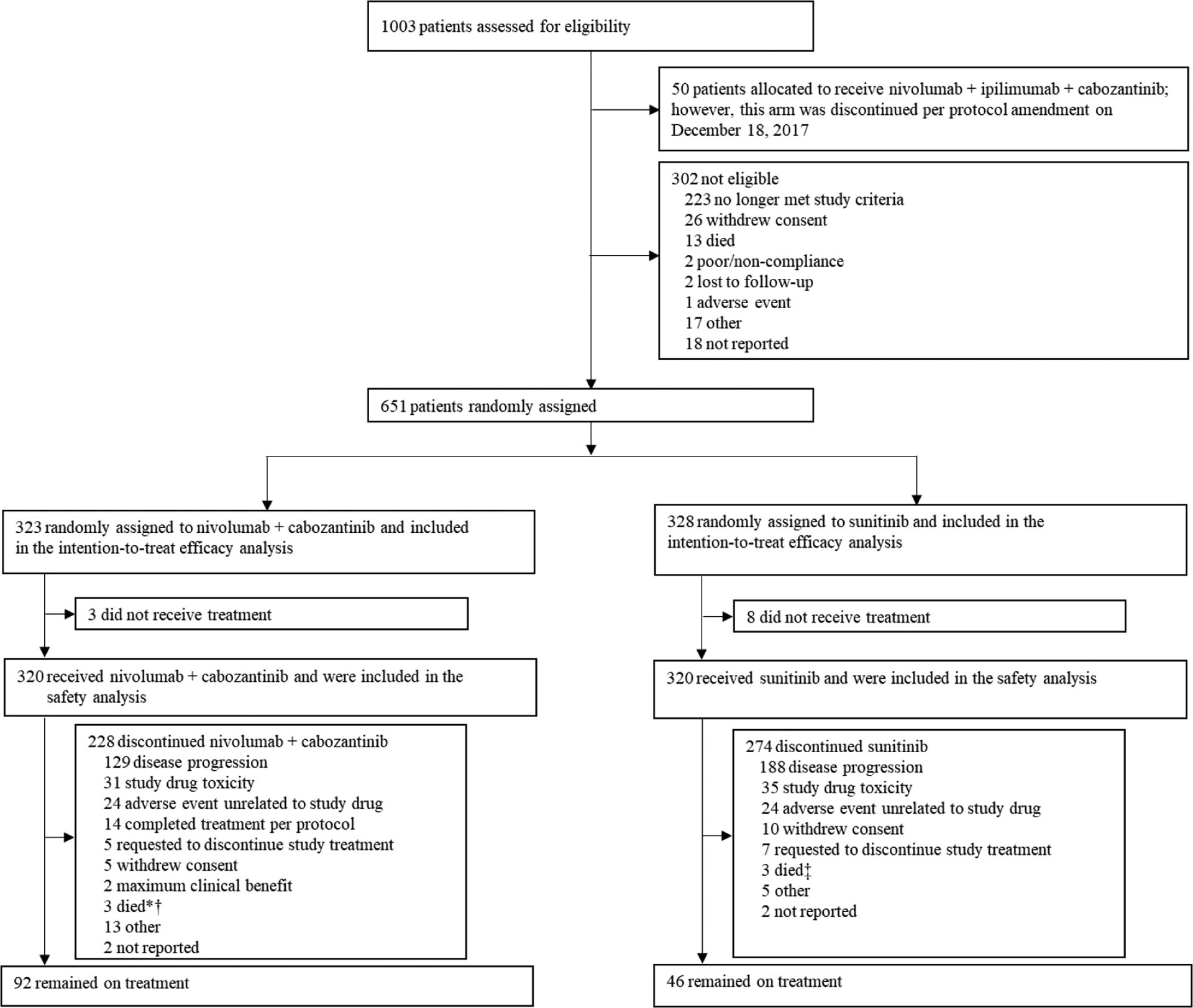
This open-label, randomised, phase 3 trial was done in 125 hospitals and cancer centres across 18 countries. We included patients aged 18 years or older with previously untreated advanced or metastatic clear-cell renal cell carcinoma, a Karnofsky performance status of 70% or higher, measurable disease according to Response Evaluation Criteria in Solid Tumors version 1.1 assessed by the investigator, any International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) prognostic risk category, and available tumour tissue for PD-L1 testing. Patients were randomly assigned (1:1) to nivolumab (240 mg) intravenously every 2 weeks plus cabozantinib (40 mg) orally once daily or sunitinib (50 mg orally) once daily (4 weeks per 6-week cycle). Randomisation, stratified by IMDC risk status, tumour PD-L1 expression, and geographical region, was done by permuted block within each stratum using a block size of four, via an interactive response system. The primary endpoint was progression-free survival by blinded independent central review. Overall survival was a secondary endpoint (reported here as the preplanned final analysis according to the protocol). Efficacy was assessed in all randomly assigned patients; safety was assessed in all patients who received at least one dose of any study drug. This ongoing study, closed to recruitment, is registered with ClinicalTrials.gov, NCT03141177.
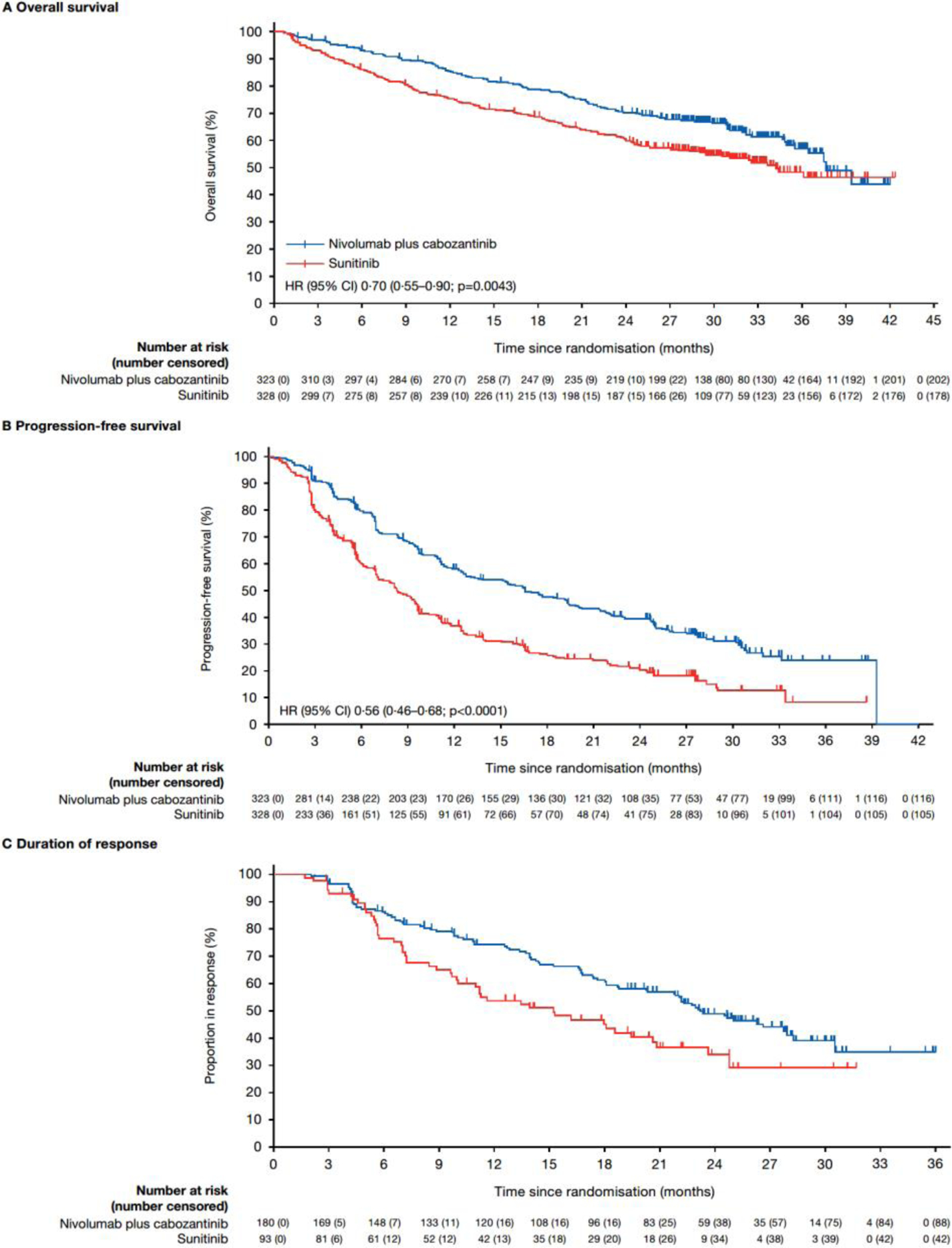
Between Sept 11, 2017, and May 14, 2019, 323 patients were randomly assigned to the nivolumab plus cabozantinib group and 328 to the sunitinib group. With an extended follow-up (data cutoff of June 24, 2021; median 32·9 months [IQR 30·4-35·9]), median overall survival was 37·7 months (95% CI 35·5-not estimable) in the nivolumab plus cabozantinib group and 34·3 months (29·0-not estimable) in the sunitinib group (hazard ratio [HR] 0·70 [95% CI 0·55-0·90], p=0·0043) and updated median progression-free survival was 16·6 months (12·8-19·8) versus 8·3 months (7·0-9·7; HR 0·56 [95% CI 0·46-0·68], p<0·0001). Grade 3-4 treatment-related adverse events occurred in 208 (65%) of 320 patients with nivolumab plus cabozantinib versus 172 (54%) of 320 with sunitinib. The most common grade 3-4 treatment-related adverse events were hypertension (40 [13%] of 320 patients in the nivolumab plus cabozantinib group vs 39 [12%] of 320 in the sunitinib group), palmar-plantar erythrodysaesthesia (25 [8%] vs 26 [8%]), and diarrhoea (22 [7%] vs 15 [5%]). Grade 3-4 treatment-related serious adverse events occurred in 70 (22%) of 320 patients in the nivolumab plus cabozantinib group and 31 (10%) of 320 in the cabozantinib group. One additional treatment-related death occurred with sunitinib (sudden death).
With extended follow-up and preplanned final overall survival analysis per protocol, nivolumab plus cabozantinib demonstrated improved efficacy versus sunitinib, further supporting the combination in the first-line treatment of advanced renal cell carcinoma.
Bristol Myers Squibb and Ono Pharmaceutical.
在 CheckMate 9ER 的主要分析中,纳武利尤单抗联合卡博替尼在未经治疗的晚期肾细胞癌患者中的无进展生存期、总生存期和客观缓解率均优于舒尼替尼(中位随访时间为 18.1 个月)。在这里,我们报告了总生存期的扩展随访以及更新的疗效和安全性数据。
这是一项在 18 个国家的 125 家医院和癌症中心进行的开放性、随机、III 期临床试验。我们纳入了年龄在 18 岁或以上、未经治疗的晚期或转移性透明细胞肾细胞癌、卡氏功能状态评分(KPS)≥70%、研究者评估的根据实体瘤反应评价标准(RECIST)1.1 可测量疾病、任何国际转移性肾细胞癌数据库联盟(IMDC)预后风险类别和可供 PD-L1 检测的肿瘤组织的患者。患者以 1:1 的比例随机分配(分层因素为 IMDC 风险状态、肿瘤 PD-L1 表达和地理区域),接受纳武利尤单抗(240mg,每 2 周静脉注射一次)联合卡博替尼(40mg,每天口服一次)或舒尼替尼(50mg,每天口服一次)(每 6 周周期中 4 周)。通过每个分层内的排列块大小为四的排列块,通过交互式响应系统进行分层随机分组。主要终点是盲法独立中央审查的无进展生存期。总生存期是次要终点(根据方案,这是预先计划的最终分析)。在所有随机分配的患者中评估疗效,在所有接受至少一剂研究药物的患者中评估安全性。这项正在进行的研究已关闭招募,在 ClinicalTrials.gov 上注册,NCT03141177。
在 2017 年 9 月 11 日至 2019 年 5 月 14 日期间,323 名患者被随机分配至纳武利尤单抗联合卡博替尼组,328 名患者被随机分配至舒尼替尼组。在延长随访(数据截止日期为 2021 年 6 月 24 日;中位随访时间为 32.9 个月[IQR 30.4-35.9])后,纳武利尤单抗联合卡博替尼组的中位总生存期为 37.7 个月(95%CI 35.5-不可估计),舒尼替尼组为 34.3 个月(29.0-不可估计)(HR 0.70[95%CI 0.55-0.90],p=0.0043),更新的中位无进展生存期为 16.6 个月(12.8-19.8)和 8.3 个月(7.0-9.7;HR 0.56[95%CI 0.46-0.68],p<0.0001)。纳武利尤单抗联合卡博替尼组 320 名患者中有 208 名(65%)发生 3-4 级治疗相关不良事件,舒尼替尼组 320 名患者中有 172 名(54%)发生 3-4 级治疗相关不良事件。最常见的 3-4 级治疗相关不良事件为高血压(纳武利尤单抗联合卡博替尼组 320 名患者中有 40 名[13%],舒尼替尼组 320 名患者中有 39 名[12%]),手掌-足底红斑感觉异常(纳武利尤单抗联合卡博替尼组 320 名患者中有 25 名[8%],舒尼替尼组 320 名患者中有 26 名[8%])和腹泻(纳武利尤单抗联合卡博替尼组 320 名患者中有 22 名[7%],舒尼替尼组 320 名患者中有 15 名[5%])。纳武利尤单抗联合卡博替尼组 320 名患者中有 70 名(22%)发生 3-4 级治疗相关严重不良事件,舒尼替尼组 320 名患者中有 31 名(10%)发生 3-4 级治疗相关严重不良事件。舒尼替尼组还发生了 1 例治疗相关死亡(猝死)。
通过扩展随访和按方案进行的最终总生存期分析,纳武利尤单抗联合卡博替尼在疗效上优于舒尼替尼,进一步支持该联合方案在晚期肾细胞癌的一线治疗中的应用。
百时美施贵宝和小野制药。