Clinical and Translational Neuroscience Unit, Department of Neurology and Feil Brain and Mind Research Institute, Weill Cornell Medicine, New York, United States.
Department of Population Health Sciences, Weill Cornell Medicine, New York, United States.
J Stroke Cerebrovasc Dis. 2022 Aug;31(8):106589. doi: 10.1016/j.jstrokecerebrovasdis.2022.106589. Epub 2022 Jun 2.
To derive models that identify patients with COVID-19 at high risk for stroke.
We used data from the AHA's Get With The Guidelines® COVID-19 Cardiovascular Disease Registry to generate models for predicting stroke risk among adults hospitalized with COVID-19 at 122 centers from March 2020-March 2021. To build our models, we used data on demographics, comorbidities, medications, and vital sign and laboratory values at admission. The outcome was a cerebrovascular event (stroke, TIA, or cerebral vein thrombosis). First, we used Cox regression with cross validation techniques to identify factors associated with the outcome in both univariable and multivariable analyses. Then, we assigned points for each variable based on corresponding coefficients to create a prediction score. Second, we used machine learning techniques to create risk estimators using all available covariates.
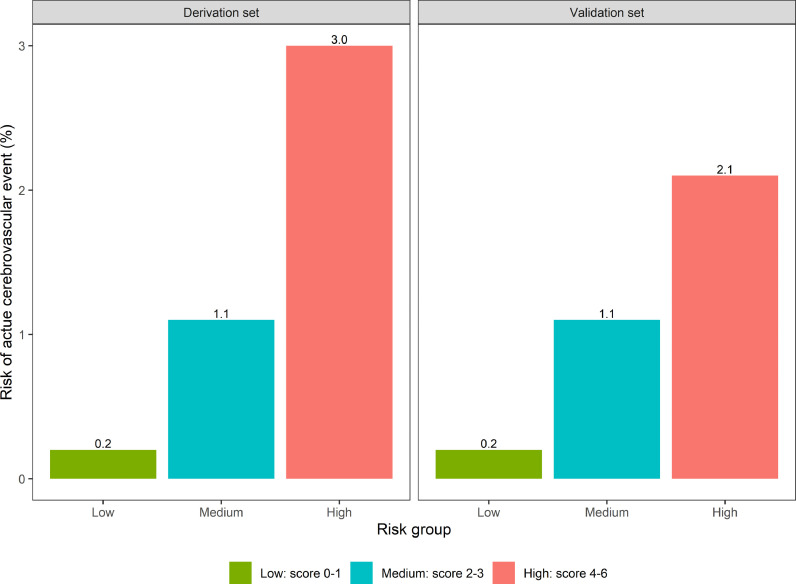
Among 21,420 patients hospitalized with COVID-19, 312 (1.5%) had a cerebrovascular event. Using traditional Cox regression, we created/validated a COVID-19 stroke risk score with a C-statistic of 0.66 (95% CI, 0.60-0.72). The CANDLE score assigns 1 point each for prior cerebrovascular disease, afebrile temperature, no prior pulmonary disease, history of hypertension, leukocytosis, and elevated systolic blood pressure. CANDLE stratified risk of an acute cerebrovascular event according to low- (0-1: 0.2% risk), medium- (2-3: 1.1% risk), and high-risk (4-6: 2.1-3.0% risk) groups. Machine learning estimators had similar discriminatory performance as CANDLE: C-statistics, 0.63-0.69.
We developed a practical clinical score, with similar performance to machine learning estimators, to help stratify stroke risk among patients hospitalized with COVID-19.
建立识别 COVID-19 患者发生卒中风险的模型。
我们使用美国心脏协会的 Get With The Guidelines® COVID-19 心血管疾病注册中心的数据,从 2020 年 3 月至 2021 年 3 月期间的 122 个中心,为因 COVID-19 住院的成年人建立预测卒中风险的模型。为了构建模型,我们使用了入院时的人口统计学、合并症、药物、生命体征和实验室值等数据。结局为脑血管事件(卒中、TIA 或脑静脉血栓形成)。首先,我们使用 Cox 回归和交叉验证技术,在单变量和多变量分析中识别与结局相关的因素。然后,我们根据相应的系数为每个变量分配分数,创建预测评分。其次,我们使用机器学习技术,使用所有可用的协变量创建风险估计器。
在因 COVID-19 住院的 21420 名患者中,有 312 名(1.5%)发生了脑血管事件。使用传统的 Cox 回归,我们创建/验证了一个 COVID-19 卒中风险评分,C 统计量为 0.66(95%CI,0.60-0.72)。CANDLE 评分对既往脑血管疾病、无发热、无既往肺部疾病、高血压史、白细胞增多症和收缩压升高各赋 1 分。CANDLE 根据低危(0-1:0.2%风险)、中危(2-3:1.1%风险)和高危(4-6:2.1-3.0%风险)组分层急性脑血管事件的风险。机器学习估计器与 CANDLE 的判别性能相似:C 统计量为 0.63-0.69。
我们开发了一种实用的临床评分,与机器学习估计器的性能相似,有助于分层 COVID-19 住院患者的卒中风险。