Division of Gastroenterology and Hepatology, Weill Cornell Medicine, New York-Presbyterian Hospital, New York, NY, United States of America.
Joan & Sanford I. Weill Medical College, Weill Cornell Medicine, New York, NY, United States of America.
PLoS One. 2020 Sep 30;15(9):e0239536. doi: 10.1371/journal.pone.0239536. eCollection 2020.
The 2019 novel coronavirus disease (COVID-19) has created unprecedented medical challenges. There remains a need for validated risk prediction models to assess short-term mortality risk among hospitalized patients with COVID-19. The objective of this study was to develop and validate a 7-day and 14-day mortality risk prediction model for patients hospitalized with COVID-19.
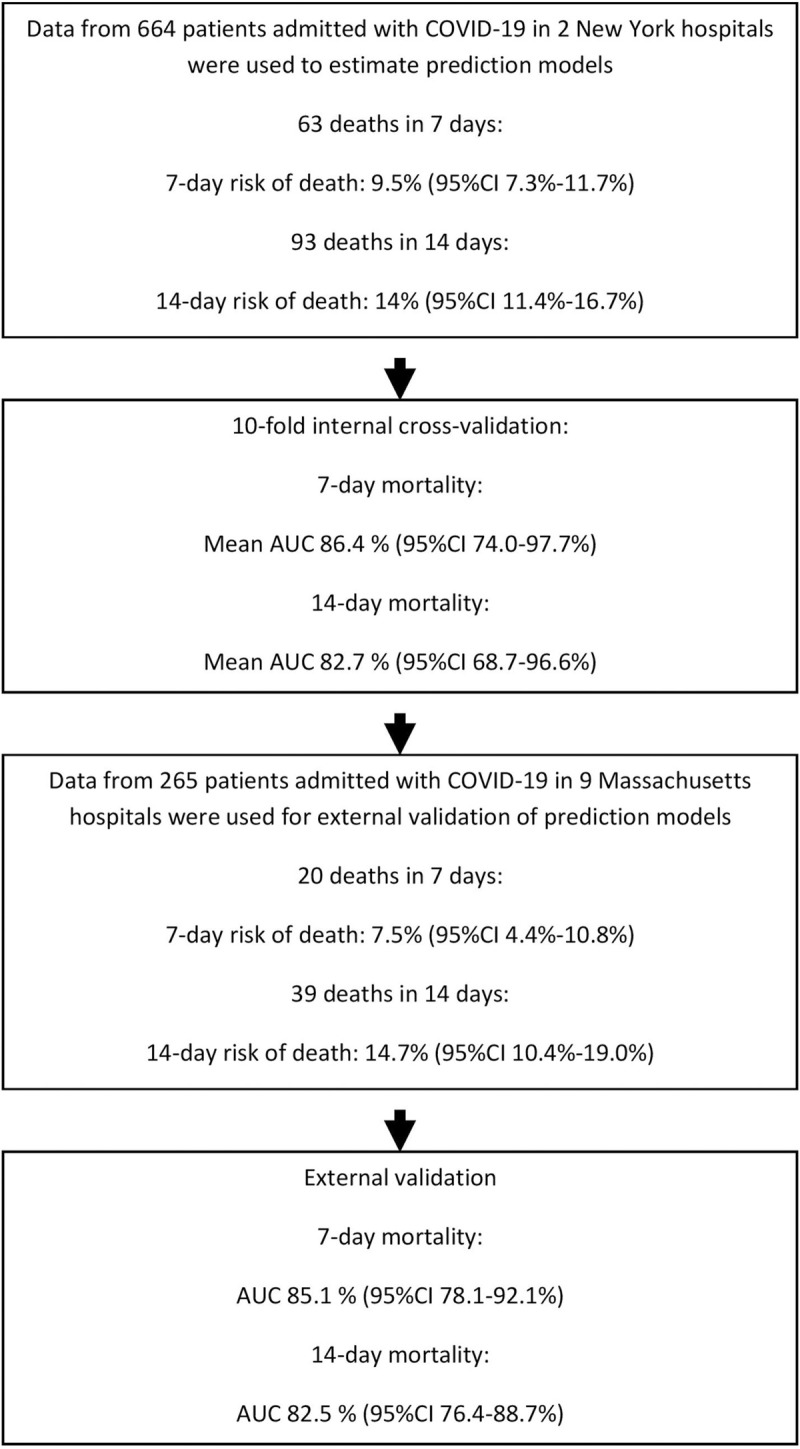
We performed a multicenter retrospective cohort study with a separate multicenter cohort for external validation using two hospitals in New York, NY, and 9 hospitals in Massachusetts, respectively. A total of 664 patients in NY and 265 patients with COVID-19 in Massachusetts, hospitalized from March to April 2020.
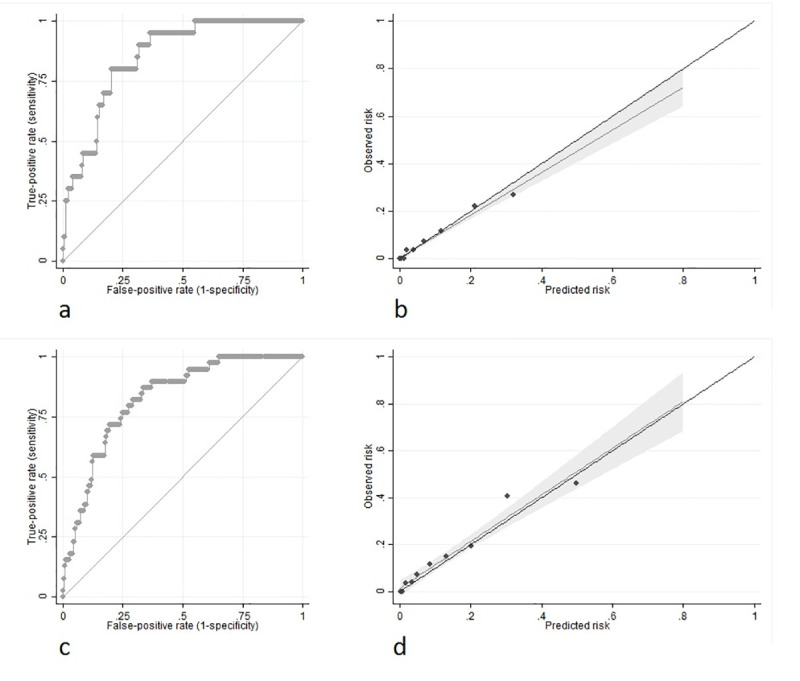
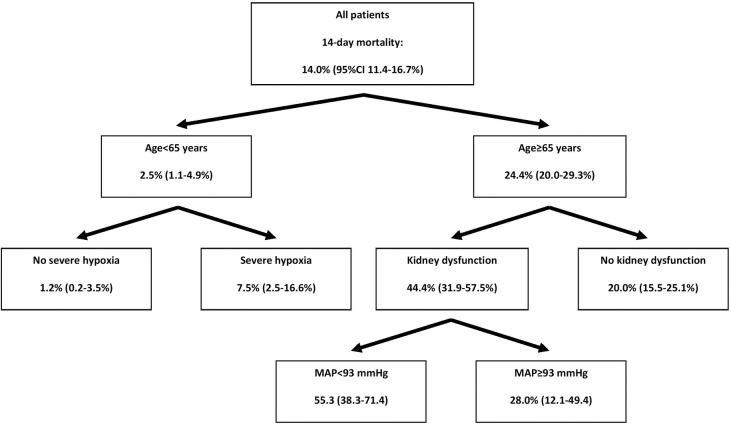
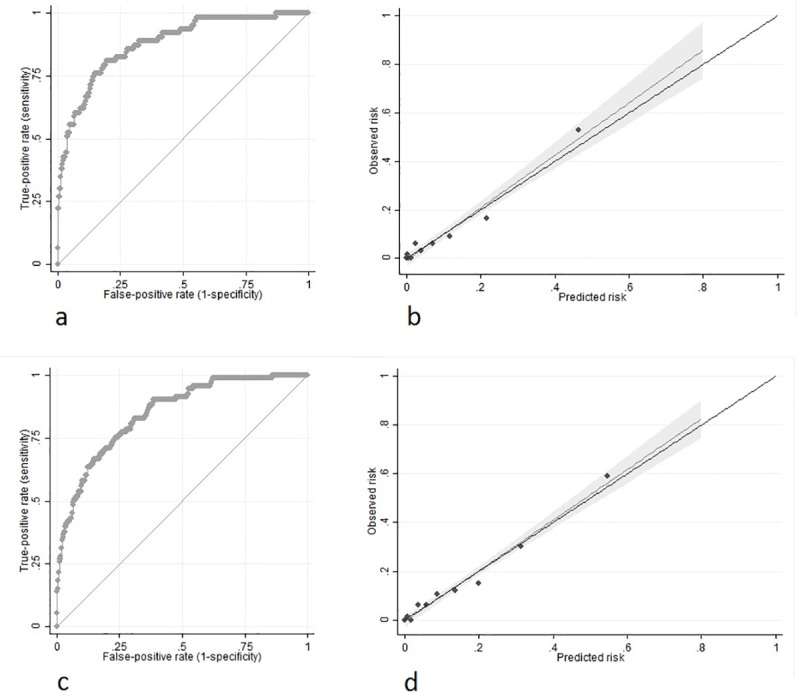
We developed a risk model consisting of patient age, hypoxia severity, mean arterial pressure and presence of kidney dysfunction at hospital presentation. Multivariable regression model was based on risk factors selected from univariable and Chi-squared automatic interaction detection analyses. Validation was by receiver operating characteristic curve (discrimination) and Hosmer-Lemeshow goodness of fit (GOF) test (calibration). In internal cross-validation, prediction of 7-day mortality had an AUC of 0.86 (95%CI 0.74-0.98; GOF p = 0.744); while 14-day had an AUC of 0.83 (95%CI 0.69-0.97; GOF p = 0.588). External validation was achieved using 265 patients from an outside cohort and confirmed 7- and 14-day mortality prediction performance with an AUC of 0.85 (95%CI 0.78-0.92; GOF p = 0.340) and 0.83 (95%CI 0.76-0.89; GOF p = 0.471) respectively, along with excellent calibration. Retrospective data collection, short follow-up time, and development in COVID-19 epicenter may limit model generalizability.
The COVID-AID risk tool is a well-calibrated model that demonstrates accuracy in the prediction of both 7-day and 14-day mortality risk among patients hospitalized with COVID-19. This prediction score could assist with resource utilization, patient and caregiver education, and provide a risk stratification instrument for future research trials.
2019 年新型冠状病毒病(COVID-19)带来了前所未有的医学挑战。仍需要经过验证的风险预测模型来评估 COVID-19 住院患者的短期死亡率风险。本研究的目的是开发和验证一种针对 COVID-19 住院患者的 7 天和 14 天死亡率风险预测模型。
我们进行了一项多中心回顾性队列研究,使用纽约的 2 家医院和马萨诸塞州的 9 家医院分别进行了外部验证。2020 年 3 月至 4 月,纽约共有 664 例患者,马萨诸塞州有 265 例 COVID-19 患者住院。
我们开发了一个风险模型,该模型由患者年龄、缺氧严重程度、平均动脉压和入院时肾功能障碍的存在组成。多变量回归模型基于单变量和卡方自动交互检测分析中选择的危险因素。验证方法为接受者操作特征曲线(区分)和 Hosmer-Lemeshow 拟合优度(GOF)检验(校准)。内部交叉验证中,7 天死亡率的预测 AUC 为 0.86(95%CI 0.74-0.98;GOF p = 0.744);而 14 天的 AUC 为 0.83(95%CI 0.69-0.97;GOF p = 0.588)。外部验证使用了来自外部队列的 265 例患者,证实了 7 天和 14 天死亡率预测的 AUC 分别为 0.85(95%CI 0.78-0.92;GOF p = 0.340)和 0.83(95%CI 0.76-0.89;GOF p = 0.471),同时具有出色的校准性能。回顾性数据收集、随访时间短以及 COVID-19 流行地区的发展可能限制了模型的通用性。
COVID-AID 风险工具是一种校准良好的模型,可准确预测 COVID-19 住院患者的 7 天和 14 天死亡率风险。该预测评分可用于辅助资源利用、患者和护理人员教育,并为未来的研究试验提供风险分层工具。