Department of Rheumatology, Kanazawa University Graduate School of Medicine, 13-1 Takaramachi, Kanazawa, Ishikawa, Japan.
Medical Education Research Center, Graduate School of Medical Sciences, Kanazawa University, 13-1 Takaramachi, Kanazawa, Ishikawa, Japan.
BMC Nephrol. 2022 Jun 11;23(1):204. doi: 10.1186/s12882-022-02835-2.
For the optimal management of patients with both allograft kidneys and native kidney diseases, the recognition of the histological features associated with older age is important. This is because most pathological findings are non-specific. Central fibrous areas (CFAs) have recently been proposed to be age-related. However, the components of CFAs and whether CFAs are observed in various kidney diseases remain undetermined. This cross-sectional study was undertaken to clarify the histological features, epidemiology, and clinicopathological features of CFAs.
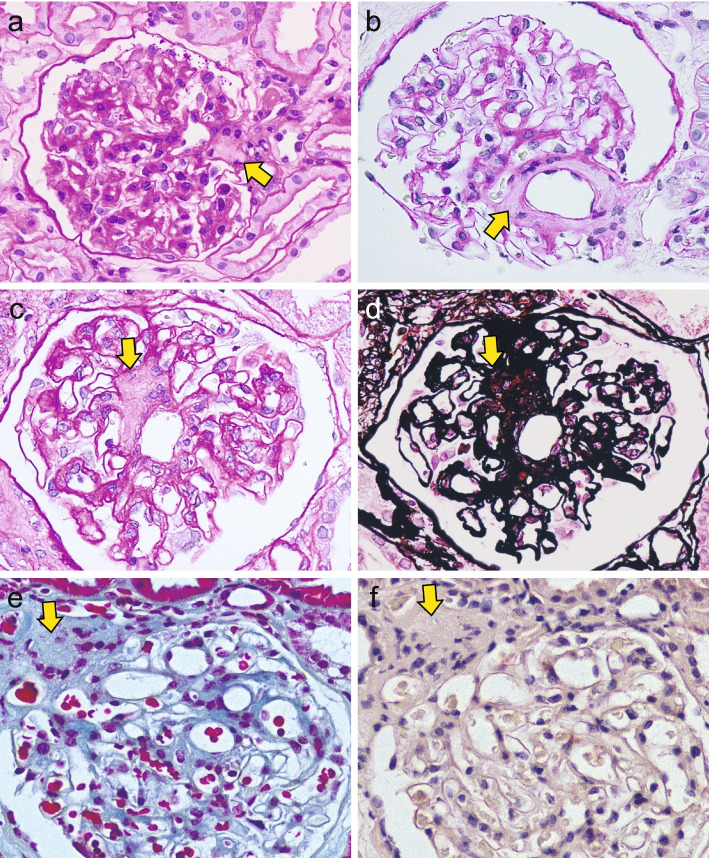
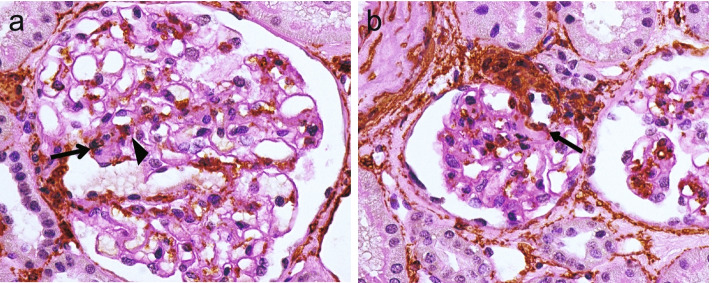
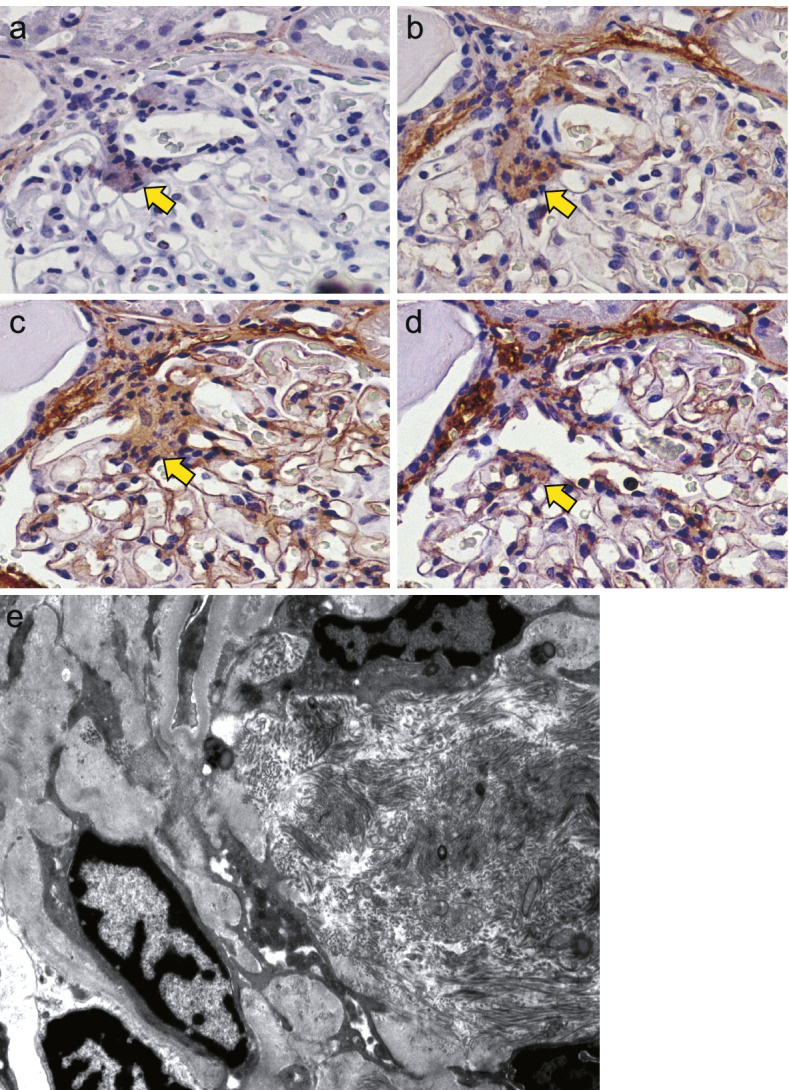
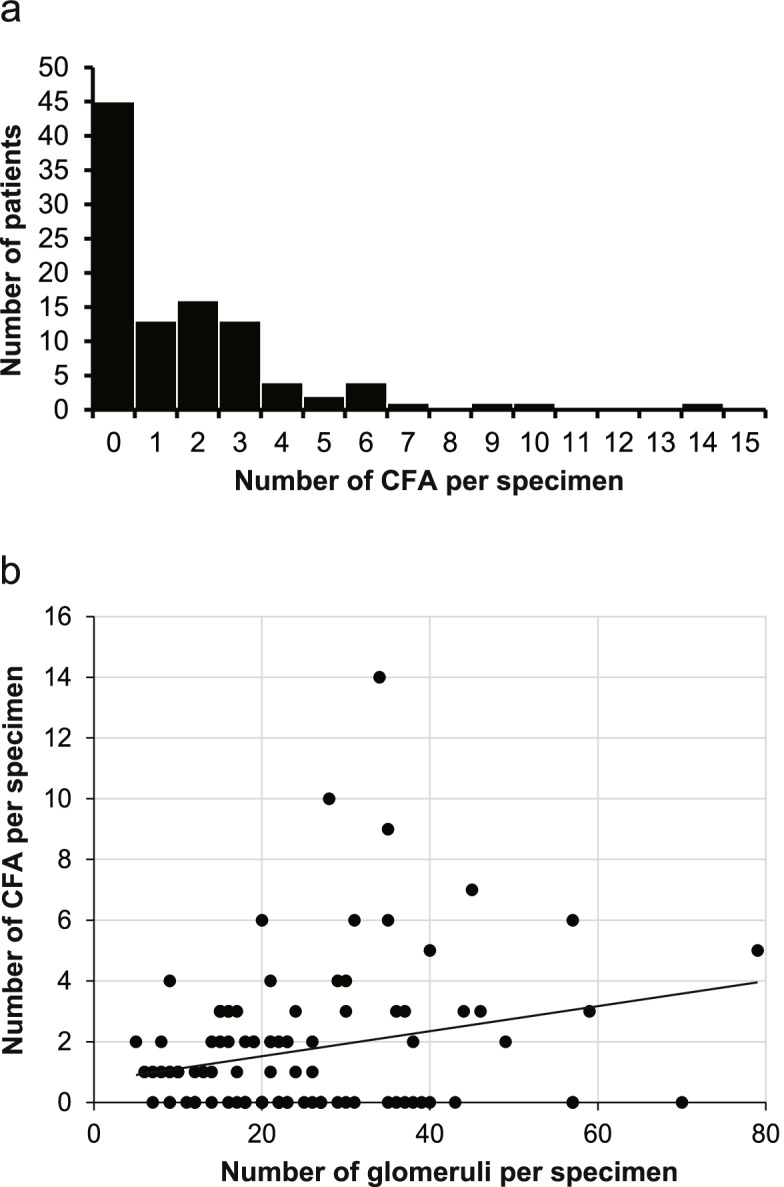
One hundred and one consecutive kidney needle biopsy specimens were retrospectively collected from seven facilities in the Hokuriku region and diagnosed at the Kanazawa University Hospital in 2015. First, the components of CFAs were analyzed using normal histostaining, immunostaining, and electron microscopy. Second, the patients were divided into two groups (CFA [+] or CFA [-]) according to the presence of CFA in the obtained samples. Clinical and histological features were compared between the two groups, and factors associated with CFA formation were determined using univariate and multivariate analyses. The number of CFAs per specimen was counted in the CFA (+) group. Third, the presence of myofibroblasts in CFA was examined by immunostaining.
CFAs were observed in 56 of 101 patients (55.4%) with various kidney diseases. CFAs consist of fibrillar collagens (collagen I and III) in addition to non-fibrillar collagens (collagen IV and VI), as confirmed by electron microscopy. Clinically, the CFA (+) group was older and had a significantly higher prevalence of hypertension and hyperlipidemia than the CFA (-) group. Histologically, elastofibrosis of the interlobular artery, arteriolar hyalinosis, and membranous nephropathy were significantly more evident in the CFA (+) group than in the CFA (-) group. Multivariate analysis revealed that older age was the sole factor associated with CFA formation. Finally, 27 of 58 (46.6%) CFA-containing glomeruli in 26 cases included alpha-smooth muscle actin-positive cells in or adjacent to the CFA.
CFAs consist of fibrous collagens in addition to matrix collagens. CFA formation is associated with older age and was observed in various kidney diseases.
为了优化同时患有同种异体肾和原生肾脏疾病患者的管理,识别与年龄相关的组织学特征非常重要。因为大多数病理发现是非特异性的。中央纤维区(CFA)最近被提出与年龄相关。然而,CFA 的组成成分以及 CFA 是否存在于各种肾脏疾病中尚不清楚。本横断面研究旨在阐明 CFA 的组织学特征、流行病学和临床病理特征。
2015 年,从北陆地区的七家医疗机构回顾性收集了 101 例连续肾脏穿刺活检标本,并在金泽大学医院进行诊断。首先,使用常规组织染色、免疫染色和电子显微镜分析 CFA 的组成成分。其次,根据获得的样本中是否存在 CFA,将患者分为 CFA[+]或 CFA[-]两组。比较两组间的临床和组织学特征,并通过单因素和多因素分析确定与 CFA 形成相关的因素。在 CFA[+]组中计算每个标本中的 CFA 数量。第三,通过免疫染色检查 CFA 中的肌成纤维细胞。
在患有各种肾脏疾病的 101 例患者中,有 56 例(55.4%)观察到 CFA。CFA 由纤维胶原(I 型和 III 型)以及非纤维胶原(IV 型和 VI 型)组成,这通过电子显微镜得到证实。临床上,CFA[+]组年龄较大,高血压和高脂血症的患病率明显高于 CFA[-]组。组织学上,CFA[+]组比 CFA[-]组更明显的弹性纤维纤维增生、小动脉玻璃样变和膜性肾病。多因素分析显示,年龄较大是与 CFA 形成相关的唯一因素。最后,在 26 例患者中,27 个包含 CFA 的肾小球(58 个肾小球中的 27 个)中,在 CFA 内或附近有 α-平滑肌肌动蛋白阳性细胞。
CFA 除基质胶原外还包含纤维胶原。CFA 的形成与年龄有关,并存在于各种肾脏疾病中。