Klingenschmid Julia, Krigers Aleksandrs, Kerschbaumer Johannes, Thomé Claudius, Pinggera Daniel, Freyschlag Christian F
Department of Neurosurgery, Medical University Innsbruck, Innsbruck, Austria.
Front Oncol. 2022 May 26;12:900382. doi: 10.3389/fonc.2022.900382. eCollection 2022.
The median age for diagnosis of glioblastoma is 64 years and the incidence rises with increasing age to a peak at 75-84 years. As the total number of high-grade glioma patients is expected to increase with an aging population, neuro-oncological surgery faces new treatment challenges, especially regarding aggressiveness of the surgical approach and extent of resection. In the elderly, aspects like frailty and functional recovery time have to be taken into account before performing surgery.
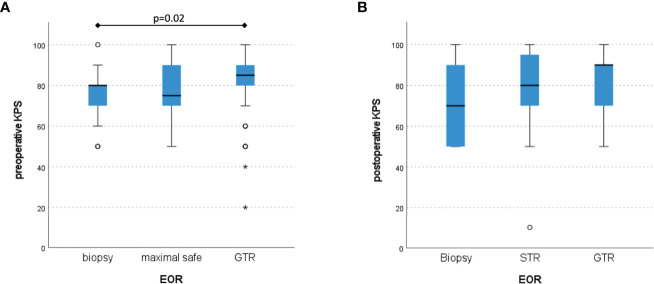
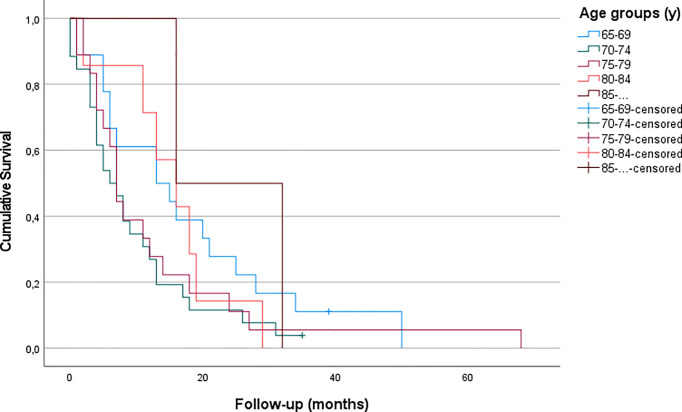
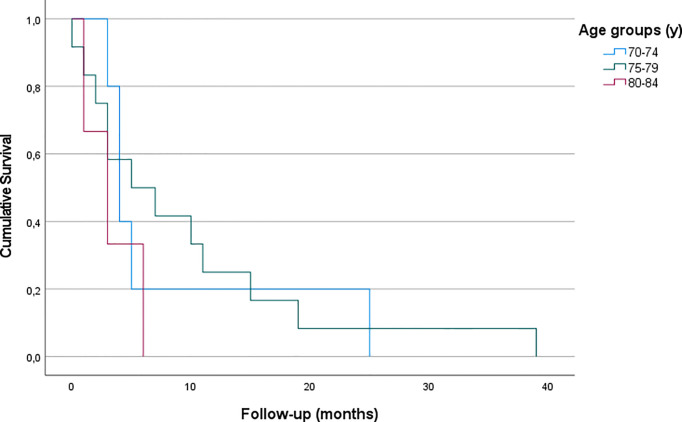
MATERIAL & METHODS: Patients undergoing surgery for malignant glioma (WHO grade III and IV) at our institution between 2015 and 2020 were compiled in a centralized tumor database and analyzed retrospectively. Karnofsky Performance Scale (KPS) and Clinical Frailty Scale (CFS) were used to determine functional performance pre- and postoperatively. Overall survival (OS) was compared between age groups of 65-69 years, 70-74 years, 75-79 years, 80-84 years and >85 years in view of extent of resection (EOR). Furthermore, we performed a literature evaluation focusing on surgical treatment of newly diagnosed malignant glioma in the elderly.
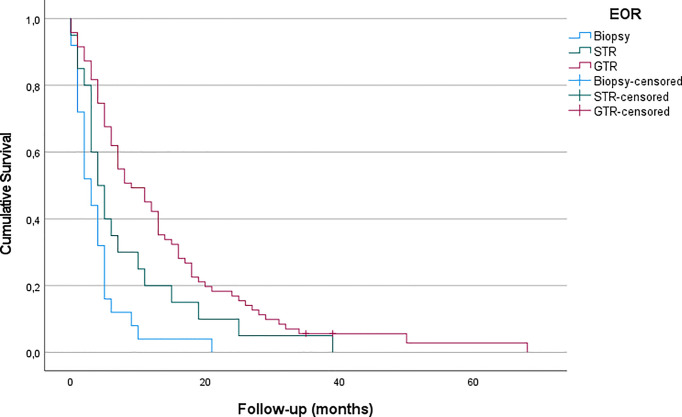
We analyzed 121 patients aged 65 years and above (range 65 to 88, mean 74 years). Mean overall survival (OS) was 10.35 months (SD = 11.38). Of all patients, only a minority (22.3%) received tumor biopsy instead of gross total resection (GTR, 61.2%) or subtotal resection (STR, 16.5%). Postoperatively, 52.9% of patients were treated according to the Stupp protocol. OS differed significantly between extent of resection (EOR) groups (4.0 months after biopsy vs. 8.3 after STR vs. 13.8 after GTR, p < 0.05 and p < 0.001 correspondingly). No significant difference was observed regarding EOR across different age groups.
GTR should be the treatment of choice also in elderly patients with malignant glioma as functional outcome and survival after surgery are remarkably better compared to less aggressive treatment. Elderly patients who received GTR of high-grade gliomas survived significantly longer compared to patients who underwent biopsy and STR. Age seems to have little influence on overall survival in selected surgically extensive treated patients, but high preoperative functional performance is mandatory.
胶质母细胞瘤的诊断中位年龄为64岁,发病率随年龄增长而上升,在75 - 84岁达到峰值。随着高级别胶质瘤患者总数预计将随着人口老龄化而增加,神经肿瘤外科面临新的治疗挑战,尤其是在手术方法的激进程度和切除范围方面。对于老年人,在进行手术前必须考虑虚弱和功能恢复时间等因素。
2015年至2020年期间在我们机构接受恶性胶质瘤(世界卫生组织III级和IV级)手术的患者被汇总到一个集中的肿瘤数据库中并进行回顾性分析。使用卡诺夫斯基功能状态量表(KPS)和临床虚弱量表(CFS)来确定术前和术后的功能表现。根据切除范围(EOR),比较了65 - 69岁、70 - 74岁、75 - 79岁、80 - 84岁和>85岁年龄组之间的总生存期(OS)。此外,我们进行了一项文献评估,重点关注老年新诊断恶性胶质瘤的手术治疗。
我们分析了121例65岁及以上的患者(年龄范围65至88岁,平均74岁)。平均总生存期(OS)为10.35个月(标准差 = 11.38)。在所有患者中,只有少数(22.3%)接受了肿瘤活检,而不是全切除(GTR,61.2%)或次全切除(STR,16.5%)。术后,52.9%的患者按照Stupp方案进行治疗。切除范围(EOR)组之间的总生存期(OS)有显著差异(活检后4.0个月,STR后8.3个月,GTR后13.8个月,相应地p < 0.05和p < 0.001)。不同年龄组之间在切除范围(EOR)方面未观察到显著差异。
对于老年恶性胶质瘤患者,全切除(GTR)也应是首选治疗方法,因为与不太激进的治疗相比,手术后的功能结果和生存期明显更好。接受高级别胶质瘤全切除(GTR)的老年患者比接受活检和次全切除(STR)的患者存活时间显著更长。在选择进行广泛手术治疗的患者中,年龄似乎对总生存期影响不大,但术前高功能状态是必需的。