Adeboyejo Kazeem, Grosche Victória Riquena, José Diego Pandeló, Ferreira Giulia Magalhães, Shimizu Jacqueline Farinha, King Barnabas J, Tarr Alexander W, Soares Márcia Maria Costa Nunes, Ball Jonathan K, McClure C Patrick, Jardim Ana Carolina Gomes
NIHR Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust and the University of Nottingham, Nottingham, UK.
School of Life Sciences, University of Nottingham, Nottingham, UK.
Access Microbiol. 2022 Mar 2;4(3):000326. doi: 10.1099/acmi.0.000326. eCollection 2022.
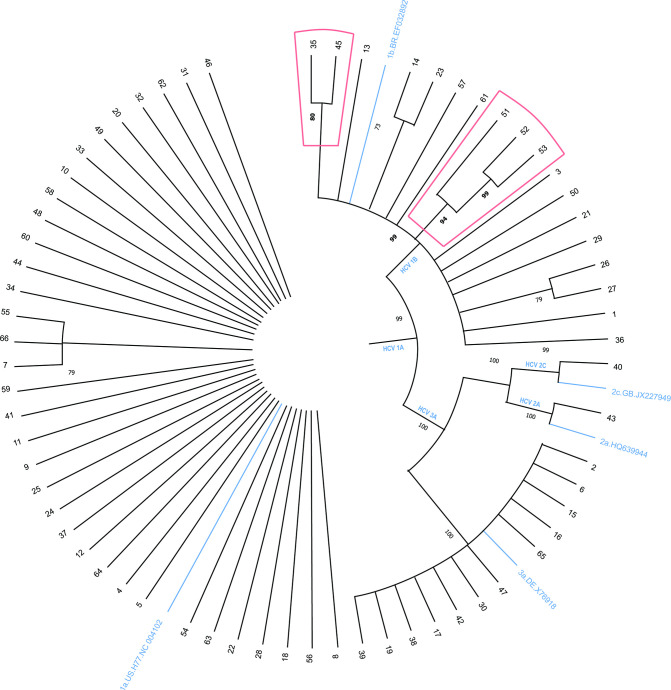
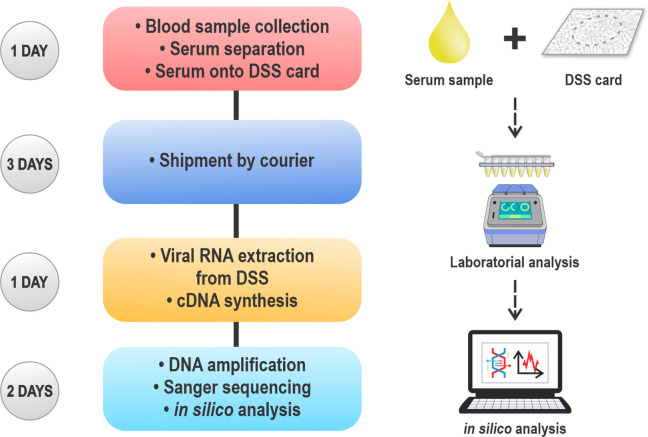
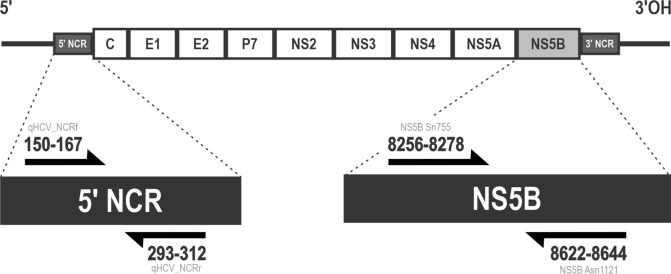
Hepatitis C virus (HCV) is responsible for more than 180 million infections worldwide, and about 80 % of infections are reported in Low and Middle-income countries (LMICs). Therapy is based on the administration of interferon (INF), ribavirin (RBV) or more recently Direct-Acting Antivirals (DAAs). However, amino acid substitutions associated with resistance (RAS) have been extensively described and can contribute to treatment failure, and diagnosis of RAS requires considerable infrastructure, not always locally available. Dried serum spots (DSS) sampling is an alternative specimen collection method, which embeds drops of serum onto filter paper to be transported by posting to a centralized laboratory. Here, we assessed feasibility of genotypic analysis of HCV from DSS in a cohort of 80 patients from São Paulo state Brazil. HCV RNA was detected on DSS specimens in 83 % of samples of HCV infected patients. HCV genotypes 1a, 1b, 2a, 2c and 3a were determined using the sequence of the palm domain of NS5B region, and RAS C316N/Y, Q309R and V321I were identified in HCV 1b samples. Concerning therapy outcome, 75 % of the patients who used INF +RBV as a previous protocol of treatment did not respond to DAAs, and 25 % were end-of-treatment responders. It suggests that therapy with INF plus RBV may contribute for non-response to a second therapeutic protocol with DAAs. One patient that presented RAS (V321I) was classified as non-responder, and combination of RAS C316N and Q309R does not necessarily imply in resistance to treatment in this cohort of patients. Data presented herein highlights the relevance of studying circulating variants for a better understanding of HCV variability and resistance to the therapy. Furthermore, the feasibility of carrying out genotyping and RAS phenotyping analysis by using DSS card for the potential of informing future treatment interventions could be relevant to overcome the limitations of processing samples in several location worldwide, especially in LMICs.
丙型肝炎病毒(HCV)在全球导致了超过1.8亿人感染,据报告约80%的感染发生在低收入和中等收入国家(LMICs)。治疗方法基于使用干扰素(INF)、利巴韦林(RBV),或者最近使用的直接抗病毒药物(DAAs)。然而,与耐药相关的氨基酸替换(RAS)已被广泛描述,并且可能导致治疗失败,而RAS的诊断需要相当多的基础设施,这些设施并非在各地都能随时获得。干血斑(DSS)采样是一种替代的样本采集方法,该方法将血清滴嵌入滤纸上,通过邮寄方式送至中央实验室。在此,我们评估了在巴西圣保罗州的80名患者队列中,从DSS进行HCV基因分型分析的可行性。在83%的HCV感染患者样本的DSS标本上检测到了HCV RNA。使用NS5B区域掌状结构域的序列确定了HCV基因型1a、1b、2a、2c和3a,并在HCV 1b样本中鉴定出了RAS C316N/Y、Q309R和V321I。关于治疗结果,75%之前使用INF + RBV作为治疗方案的患者对DAAs无反应,25%为治疗结束时的有反应者。这表明使用INF加RBV进行治疗可能导致对DAAs的第二种治疗方案无反应。一名出现RAS(V321I)的患者被归类为无反应者,并且在该患者队列中,RAS C316N和Q309R的组合并不一定意味着对治疗耐药。本文提供的数据突出了研究循环变异体对于更好地理解HCV变异性和治疗耐药性的重要性。此外,使用DSS卡进行基因分型和RAS表型分析的可行性,因其对未来治疗干预具有潜在的指导作用,可能有助于克服在全球多个地点处理样本的局限性,尤其是在低收入和中等收入国家。