Chen Xiaomeng, Chu Nadia M, Basyal Pragyashree Sharma, Vihokrut Wasurut, Crews Deidra, Brennan Daniel C, Andrews Sarah R, Vannorsdall Tracy D, Segev Dorry L, McAdams-DeMarco Mara A
Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA.
Kidney Int Rep. 2022 Mar 15;7(6):1306-1317. doi: 10.1016/j.ekir.2022.03.008. eCollection 2022 Jun.
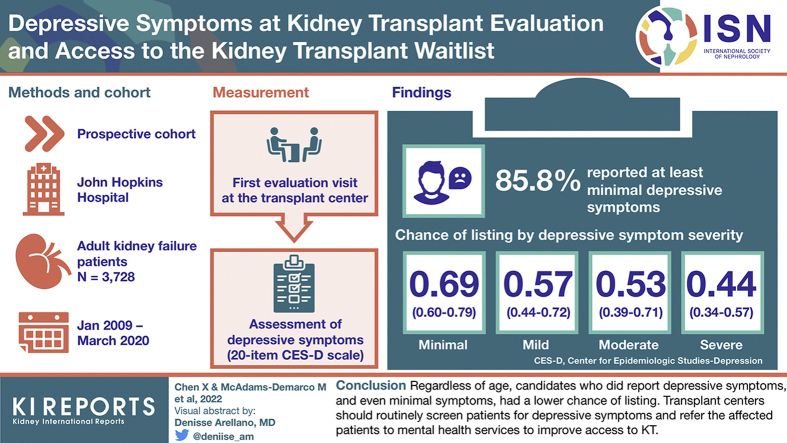
Depressive symptoms, even without a clinical diagnosis of depression, are common in kidney failure patients and may be a barrier to completing the complex process of kidney transplant (KT) evaluation. We assessed depressive symptom burden and association between depressive symptoms and access to KT waitlist by age.
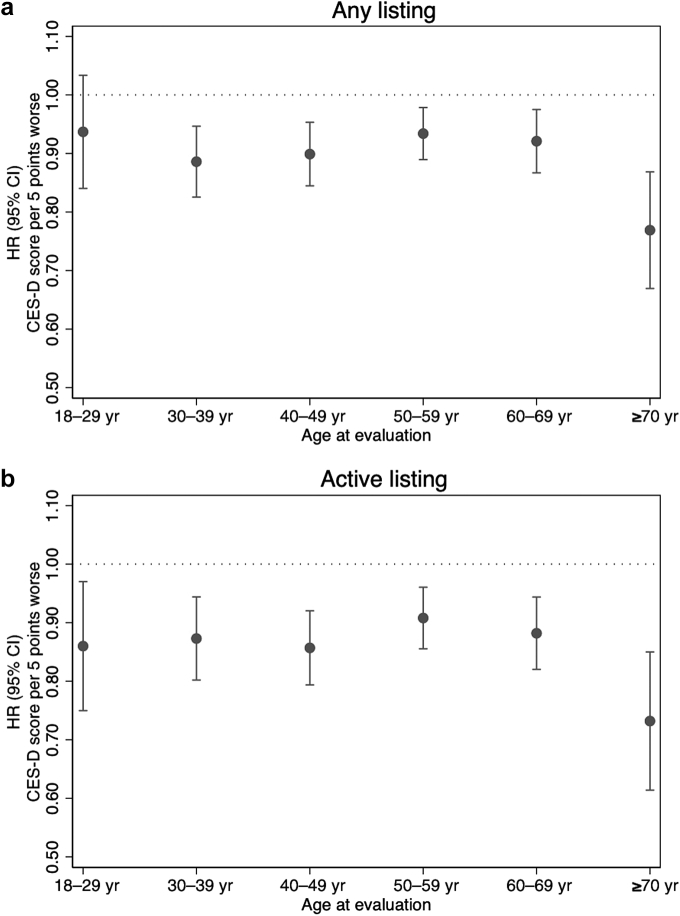
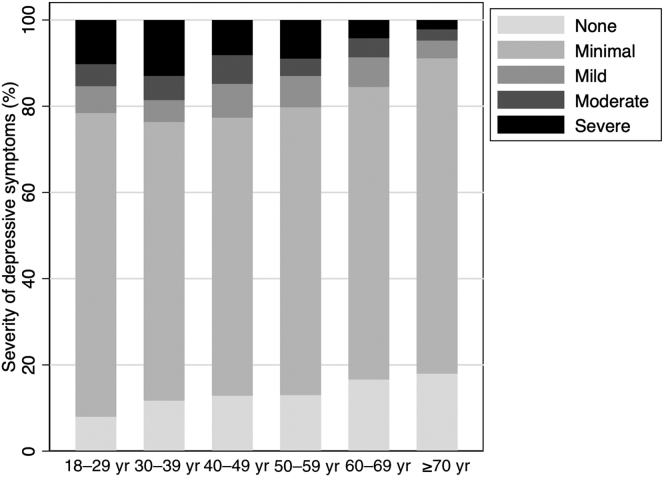
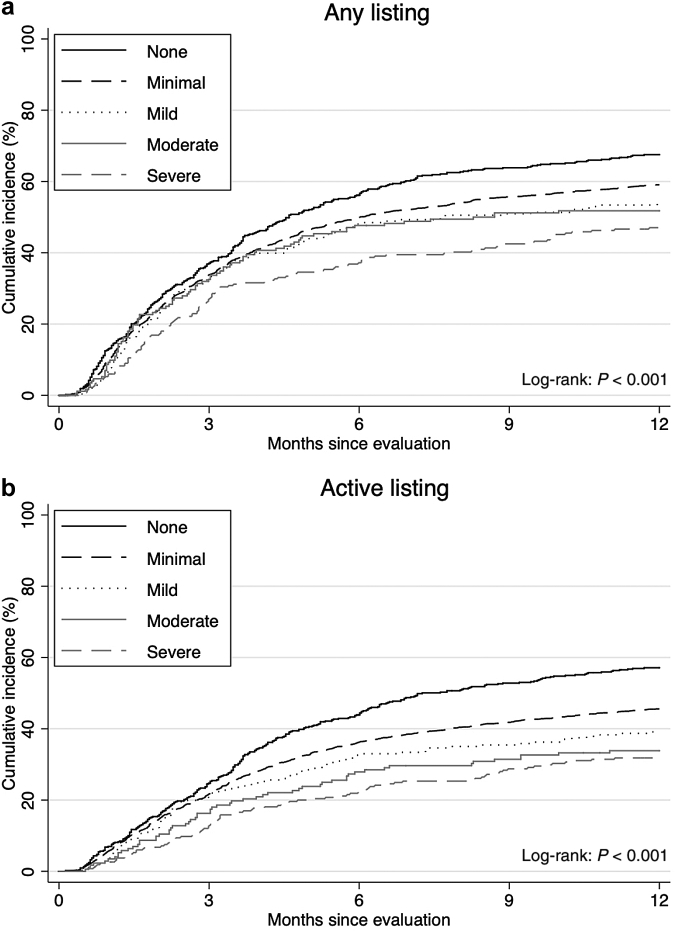
In a prospective cohort of 3728 KT patients (aged 18-88 years), the Center for Epidemiologic Studies-Depression (CES-D) scale was used to measure depressive symptoms at evaluation. Depressive symptom severity was defined as follows: none: 0; minimal: 1 to 15; mild: 16 to 20; moderate: 21 to 25; severe: 26 to 60. Hazard ratios (HRs) of active listing within 1 year after evaluation were estimated using Cox proportional hazards models, adjusted for clinical and social factors.
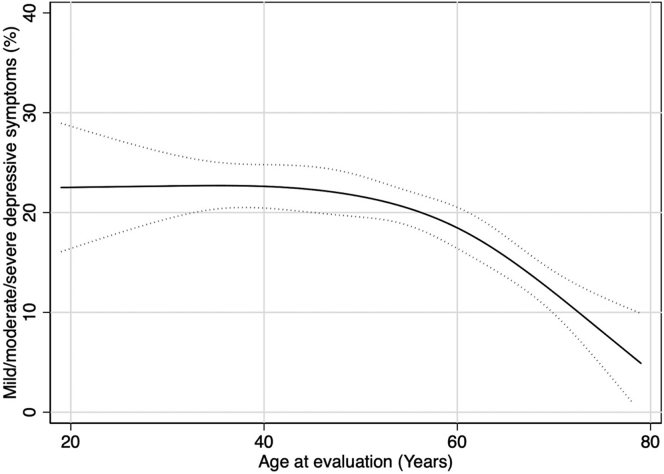
At evaluation, 85.8% of the patients reported at least minimal depressive symptoms; the proportion was lower among older patients: 18 to 29 years = 92.0%; 30 to 39 years = 88.3%; 40 to 49 years = 87.2%; 50 to 59 years = 87.0%; 60 to 69 years = 83.4%; and ≥70 years = 82.0%. Chance of active listing decreased with more severe depressive symptoms (log-rank, < 0.001). After adjustment, every 5-point higher CES-D score (more depressive symptoms) was associated with a 13% lower chance of listing (HR = 0.87, 95% CI: 0.85-0.90); the strongest association was found among patients aged ≥70 years (adjusted HR [aHR] = 0.73, 95% CI: 0.62-0.86). Furthermore, minimal (HR = 0.69, 95% CI: 0.60-0.79), mild (HR = 0.57, 95% CI: 0.44-0.72), moderate (HR = 0.53, 95% CI: 0.39-0.71), and severe (HR = 0.44, 95% CI: 0.34-0.57) depressive symptoms were all associated with a lower chance of listing.
Older candidates were less likely to report depressive symptoms at KT evaluation. Regardless of age, candidates who did report depressive symptoms, and even minimal symptoms, had a lower chance of listing. Transplant centers should routinely screen patients for depressive symptoms and refer the affected patients to mental health services to improve access to KT.
抑郁症状在肾衰竭患者中很常见,即使没有临床诊断为抑郁症,也可能成为完成复杂的肾移植(KT)评估过程的障碍。我们评估了抑郁症状负担以及抑郁症状与按年龄分组获得KT等待名单之间的关联。
在一个由3728名KT患者(年龄在18 - 88岁之间)组成的前瞻性队列中,使用流行病学研究中心抑郁量表(CES - D)在评估时测量抑郁症状。抑郁症状严重程度定义如下:无:0分;轻微:1至15分;轻度:16至20分;中度:21至25分;重度:26至60分。使用Cox比例风险模型估计评估后1年内进入活动名单的风险比(HR),并对临床和社会因素进行调整。
在评估时,85.8%的患者报告至少有轻微抑郁症状;老年患者中的比例较低:18至29岁 = 92.0%;30至39岁 = 88.3%;40至49岁 = 87.2%;50至59岁 = 87.0%;60至69岁 = 83.4%;≥70岁 = 82.0%。抑郁症状越严重,进入活动名单的机会越低(对数秩检验,< 0.001)。调整后,CES - D评分每升高5分(抑郁症状更严重)与进入名单的机会降低13%相关(HR = 0.87,95%置信区间:0.85 - 0.90);在≥70岁的患者中发现最强的关联(调整后HR [aHR] = 0.73,95%置信区间:0.62 - 0.86)。此外,轻微(HR = 0.69,95%置信区间:0.60 - 0.79)、轻度(HR = 0.57,95%置信区间:0.44 - 0.72)、中度(HR = 0.53,95%置信区间:0.39 - 0.71)和重度(HR = 0.44,95%置信区间:0.34 - 0.57)抑郁症状均与进入名单的机会降低相关。
老年候选人在KT评估时报告抑郁症状的可能性较小。无论年龄如何,报告有抑郁症状甚至轻微症状的候选人进入名单的机会较低。移植中心应常规筛查患者的抑郁症状,并将受影响的患者转介至心理健康服务机构,以改善获得KT的机会。