Centre of Clinical Research Femme Enfant Adolescent, Hôpital Femme Enfant Adolescent, Inserm 1413, CHU de Nantes, Nantes, France.
Inserm UMR 1153, Obstetrical, Perinatal and Pediatric Epidemiology Research Team (Epopé), Centre of Research in Epidemiology and Statistics, Université Paris Cité, Paris, France.
JAMA Netw Open. 2022 Jun 1;5(6):e2216778. doi: 10.1001/jamanetworkopen.2022.16778.
Assessment of the quality of initial care is necessary to target priority actions that can reduce the still high morbidity and mortality due to community-onset severe bacterial infections (COSBIs) among children.
To study the prevalence, characteristics, and determinants of suboptimal care in the initial management of COSBIs.
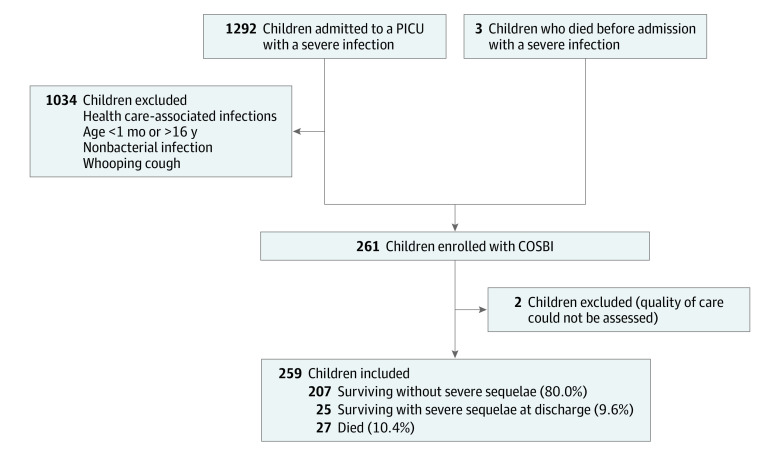
DESIGN, SETTING, AND PARTICIPANTS: This prospective, population-based, cohort study and confidential enquiry was conducted between August 2009 and January 2014 in western France, a region accounting for 15% of the French pediatric population (1 968 474 children aged 1 month to 16 years) and including 6 pediatric intensive care units (PICUs) and 35 emergency departments. Participants included all children aged 1 month to 16 years who died before PICU admission or were admitted to a PICU with a COSBI (ie, bacterial sepsis, including meningitis, purpura fulminans, and pulmonary, osteoarticular, intra-abdominal, cardiac, and soft-tissue severe infections). Data were analyzed from March to June 2020.
Suboptimal care determined according to evaluation of 8 types of care: (1) the delay in seeking care by family, (2) the physician's evaluation of severity, (3) the patient's referral at the first consultation with signs of severity, (4) the timing and (5) dosage of antibiotic treatment, (6) the timing and (7) volume of fluid bolus administration, and (8) the clinical reassessment after fluid bolus.
Two experts assessed the quality of care before death or PICU admission as optimal, possibly suboptimal, or certainly suboptimal. The consequences and determinants of certainly suboptimal care were identified with multinomial logistic regression and generalized linear mixed models.
Of the 259 children included (median [IQR] age, 24 [6-66] months; 143 boys [55.2%]), 27 (10.4%) died, and 25 (9.6%) had severe sequelae at PICU discharge. The quality of care was certainly suboptimal in 89 cases (34.4%). Suboptimal care was more frequent in children with sequelae (adjusted odds ratio [aOR], 5.61; 95% CI, 1.19-26.36) and less frequent in children who died (aOR, 0.16; 95% CI, 0.04-0.65) vs those surviving without sequelae. Factors independently associated with suboptimal care were age younger than 5 years (aOR, 3.15; 95% CI, 1.25-7.90), diagnosis of sepsis with no source (aOR, 5.77; 95% CI, 1.64-20.30) or meningitis (aOR, 3.39; 95% CI, 1.15-9.96) vs other severe infections, and care by a primary care physician (aOR, 3.22; 95% CI, 1.17-8.88) vs a pediatric hospital service.
This study found that suboptimal care is frequent in the initial management of COSBI and is associated with severe sequelae. The paradoxical association with reduced risk of death may be explained by an insufficient adjustment on bacterial or host intrinsic factors. Management could be optimized by improving the quality of primary care, especially for young children.
评估初始治疗的质量对于确定优先行动是必要的,这些行动可以降低儿童社区获得性严重细菌感染(COSBIs)的高发病率和死亡率。
研究 COSBIs 初始管理中治疗不足的流行情况、特征和决定因素。
设计、地点和参与者:这是一项前瞻性、基于人群的队列研究和机密调查,于 2009 年 8 月至 2014 年 1 月在法国西部进行,该地区占法国儿科人口的 15%(1968474 名 1 个月至 16 岁的儿童),包括 6 个儿科重症监护病房(PICUs)和 35 个急诊部门。参与者包括所有在进入 PICU 之前死亡或因 COBSI 而入住 PICU 的 1 个月至 16 岁的儿童(即细菌败血症,包括脑膜炎、暴发性紫癜、肺部、骨关节炎、腹内、心脏和软组织严重感染)。数据于 2020 年 3 月至 6 月进行分析。
根据 8 种护理类型的评估确定的治疗不足:(1)家庭寻求护理的延迟,(2)医生对严重程度的评估,(3)患者在出现严重症状的首次就诊时转诊,(4)抗生素治疗的时间和(5)剂量,(6)输液量的时间和(7),(8)输液后临床重新评估。
两名专家在死亡或 PICU 入院前评估护理质量为最佳、可能治疗不足或肯定治疗不足。使用多项逻辑回归和广义线性混合模型确定肯定治疗不足的后果和决定因素。
在 259 名纳入的儿童中(中位数[IQR]年龄,24[6-66]个月;143 名男孩[55.2%]),27 名(10.4%)死亡,25 名(9.6%)在 PICU 出院时出现严重后遗症。89 例(34.4%)的护理质量肯定不足。在有后遗症的儿童中,治疗不足更为常见(调整后优势比[aOR],5.61;95%CI,1.19-26.36),在没有后遗症且存活的儿童中则较少(aOR,0.16;95%CI,0.04-0.65)。与治疗不足相关的独立因素包括年龄小于 5 岁(aOR,3.15;95%CI,1.25-7.90)、无来源的败血症诊断(aOR,5.77;95%CI,1.64-20.30)或脑膜炎(aOR,3.39;95%CI,1.15-9.96)与其他严重感染相比,以及由初级保健医生治疗(aOR,3.22;95%CI,1.17-8.88)与儿科医院服务相比。
这项研究发现,COSBIs 初始管理中的治疗不足很常见,并且与严重后遗症有关。与死亡风险降低相关的矛盾关联可能是由于细菌或宿主内在因素的调整不足所致。通过提高初级保健的质量,特别是为幼儿提供更好的治疗,可以优化管理。