MacKenna Brian, Kennedy Nicholas A, Mehrkar Amir, Rowan Anna, Galloway James, Matthewman Julian, Mansfield Kathryn E, Bechman Katie, Yates Mark, Brown Jeremy, Schultze Anna, Norton Sam, Walker Alex J, Morton Caroline E, Harrison David, Bhaskaran Krishnan, Rentsch Christopher T, Williamson Elizabeth, Croker Richard, Bacon Seb, Hickman George, Ward Tom, Davy Simon, Green Amelia, Fisher Louis, Hulme William, Bates Chris, Curtis Helen J, Tazare John, Eggo Rosalind M, Evans David, Inglesby Peter, Cockburn Jonathan, McDonald Helen I, Tomlinson Laurie A, Mathur Rohini, Wong Angel Y S, Forbes Harriet, Parry John, Hester Frank, Harper Sam, Douglas Ian J, Smeeth Liam, Lees Charlie W, Evans Stephen J W, Goldacre Ben, Smith Catherine H, Langan Sinéad M
The Bennett Institute for Applied Data Science, Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Department of Gastroenterology, Royal Devon and Exeter NHS Foundation Trust, Exeter, UK.
Lancet Rheumatol. 2022 Jul;4(7):e490-e506. doi: 10.1016/S2665-9913(22)00098-4. Epub 2022 Jun 9.
The risk of severe COVID-19 outcomes in people with immune-mediated inflammatory diseases and on immune-modifying drugs might not be fully mediated by comorbidities and might vary by factors such as ethnicity. We aimed to assess the risk of severe COVID-19 in adults with immune-mediated inflammatory diseases and in those on immune-modifying therapies.
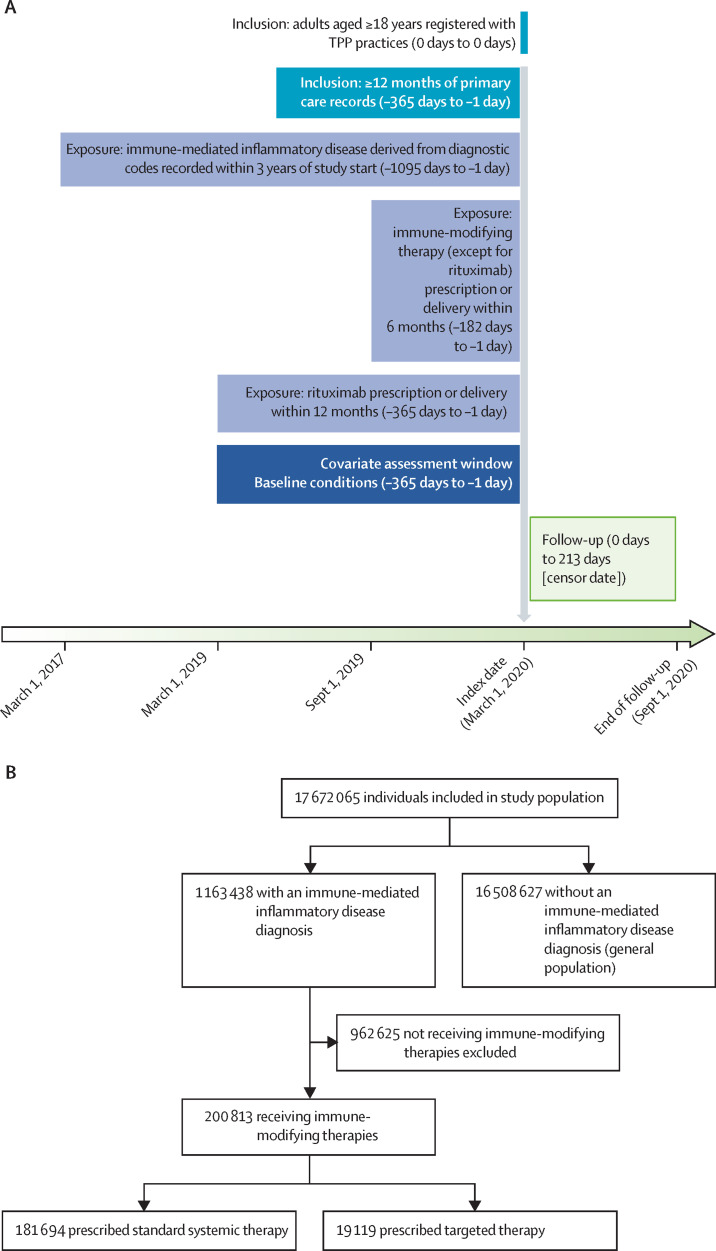
We did a cohort study, using OpenSAFELY (an analytics platform for electronic health records) and TPP (a software provider for general practitioners), analysing routinely collected primary care data linked to hospital admission, death, and previously unavailable hospital prescription data. We included people aged 18 years or older on March 1, 2020, who were registered with TPP practices with at least 12 months of primary care records before March, 2020. We used Cox regression (adjusting for confounders and mediators) to estimate hazard ratios (HRs) comparing the risk of COVID-19-related death, critical care admission or death, and hospital admission (from March 1 to Sept 30, 2020) in people with immune-mediated inflammatory diseases compared with the general population, and in people with immune-mediated inflammatory diseases on targeted immune-modifying drugs (eg, biologics) compared with those on standard systemic treatment (eg, methotrexate).
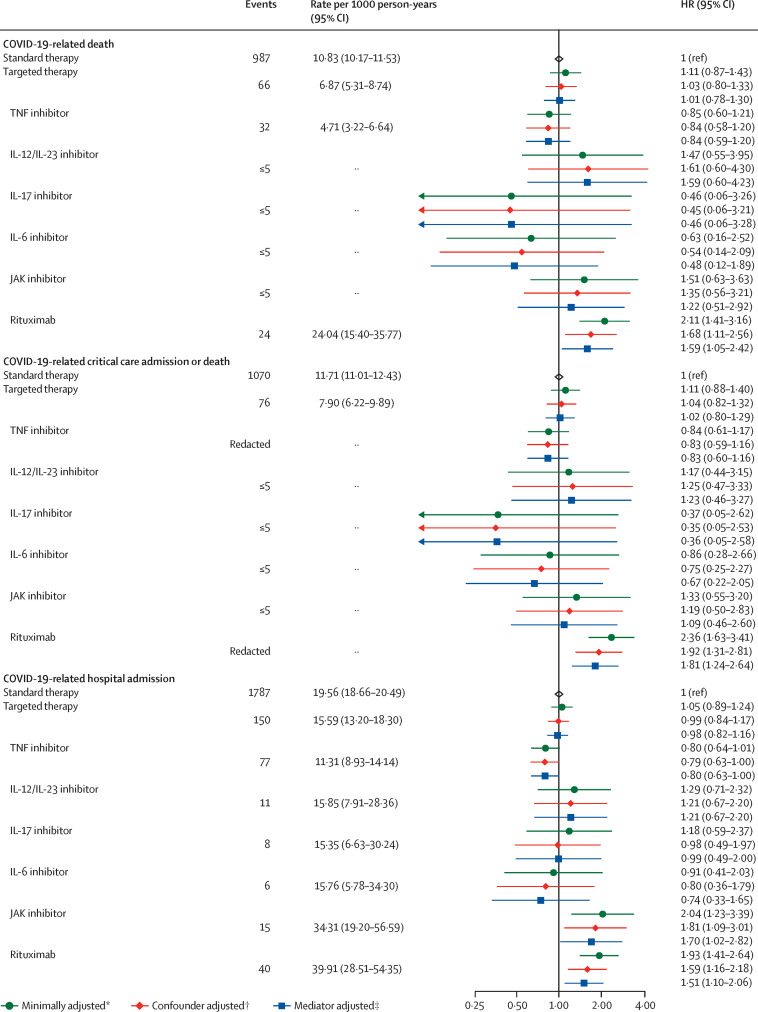
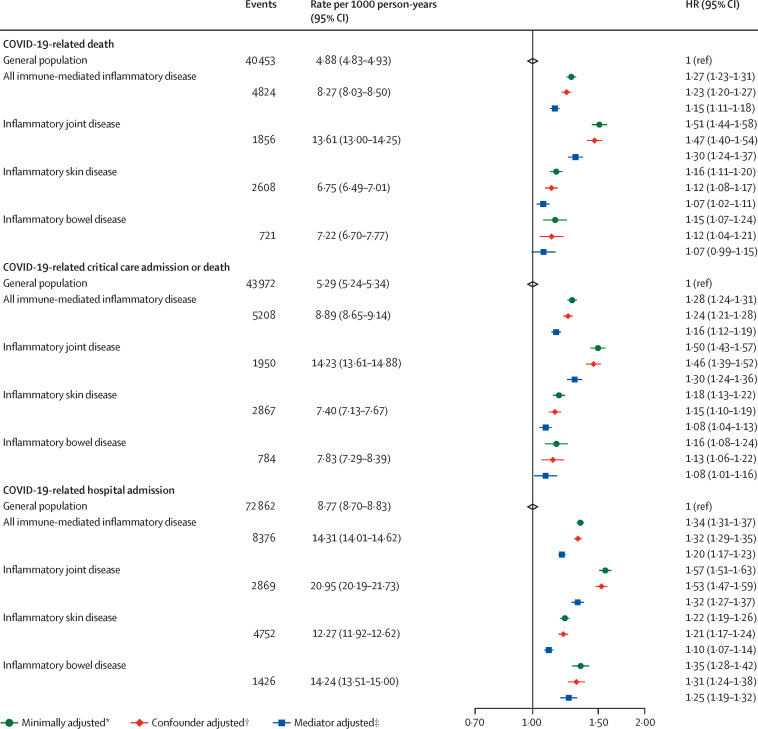
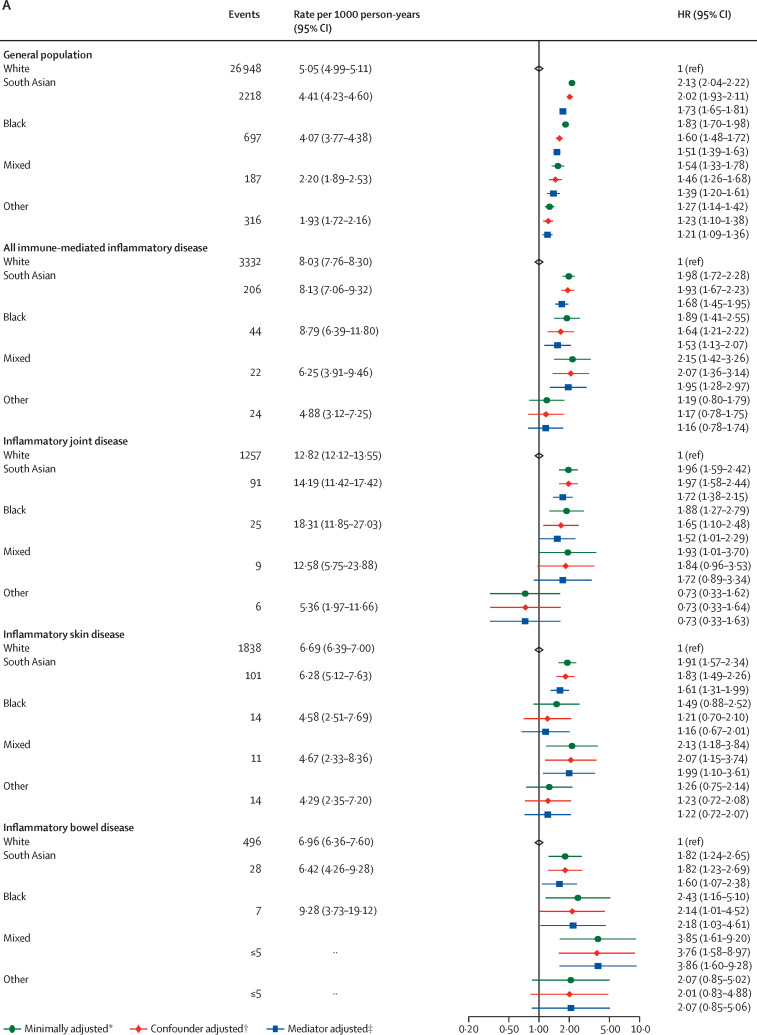
We identified 17 672 065 adults; 1 163 438 adults (640 164 [55·0%] women and 523 274 [45·0%] men, and 827 457 [71·1%] of White ethnicity) had immune-mediated inflammatory diseases, and 16 508 627 people (8 215 020 [49·8%] women and 8 293 607 [50·2%] men, and 10 614 096 [64·3%] of White ethnicity) were included as the general population. Of 1 163 438 adults with immune-mediated inflammatory diseases, 19 119 (1·6%) received targeted immune-modifying therapy and 181 694 (15·6%) received standard systemic therapy. Compared with the general population, adults with immune-mediated inflammatory diseases had an increased risk of COVID-19-related death after adjusting for confounders (age, sex, deprivation, and smoking status; HR 1·23, 95% CI 1·20-1·27) and further adjusting for mediators (body-mass index [BMI], cardiovascular disease, diabetes, and current glucocorticoid use; 1·15, 1·11-1·18). Adults with immune-mediated inflammatory diseases also had an increased risk of COVID-19-related critical care admission or death (confounder-adjusted HR 1·24, 95% CI 1·21-1·28; mediator-adjusted 1·16, 1·12-1·19) and hospital admission (confounder-adjusted 1·32, 1·29-1·35; mediator-adjusted 1·20, 1·17-1·23). In post-hoc analyses, the risk of severe COVID-19 outcomes in people with immune-mediated inflammatory diseases was higher in non-White ethnic groups than in White ethnic groups (as it was in the general population). We saw no evidence of increased COVID-19-related death in adults on targeted, compared with those on standard systemic, therapy after adjusting for confounders (age, sex, deprivation, BMI, immune-mediated inflammatory diseases [bowel, joint, and skin], cardiovascular disease, cancer [excluding non-melanoma skin cancer], stroke, and diabetes (HR 1·03, 95% CI 0·80-1·33), and after additionally adjusting for current glucocorticoid use (1·01, 0·78-1·30). There was no evidence of increased COVID-19-related death in adults prescribed tumour necrosis factor inhibitors, interleukin (IL)-12/IL‑23 inhibitors, IL-17 inhibitors, IL-6 inhibitors, or Janus kinase inhibitors compared with those on standard systemic therapy. Rituximab was associated with increased COVID-19-related death (HR 1·68, 95% CI 1·11-2·56), with some attenuation after excluding people with haematological malignancies or organ transplants (1··-·).
COVID-19 deaths and hospital admissions were higher in people with immune-mediated inflammatory diseases. We saw no increased risk of adverse COVID-19 outcomes in those on most targeted immune-modifying drugs for immune-mediated inflammatory diseases compared with those on standard systemic therapy.
UK Medical Research Council, NIHR Biomedical Research Centre at King's College London and Guy's and St Thomas' NHS Foundation Trust, and Wellcome Trust.
免疫介导的炎症性疾病患者以及使用免疫调节药物的人群发生重症 COVID-19 结局的风险可能并非完全由合并症介导,且可能因种族等因素而异。我们旨在评估患有免疫介导的炎症性疾病的成年人以及接受免疫调节治疗的人群发生重症 COVID-19 的风险。
我们进行了一项队列研究,使用 OpenSAFELY(一个电子健康记录分析平台)和 TPP(一家全科医生软件提供商),分析与住院、死亡以及之前无法获取的医院处方数据相关的常规收集的初级保健数据。我们纳入了 2020 年 3 月 1 日及以上、在 2020 年 3 月之前在 TPP 诊所注册且有至少 12 个月初级保健记录的人群。我们使用 Cox 回归(对混杂因素和中介因素进行调整)来估计风险比(HRs),比较免疫介导的炎症性疾病患者与普通人群相比发生 COVID-19 相关死亡、重症监护入院或死亡以及住院(2020 年 3 月 1 日至 9 月 30 日)的风险,以及使用靶向免疫调节药物(如生物制剂)的免疫介导的炎症性疾病患者与使用标准全身治疗(如甲氨蝶呤)的患者相比的风险。
我们识别出 17672065 名成年人;1163438 名成年人(640164[55.0%]为女性,523274[45.0%]为男性,827457[71.1%]为白人)患有免疫介导的炎症性疾病,16508627 人(8215020[49.8%]为女性,8293607[50.2%]为男性,10614096[64.3%]为白人)被纳入作为普通人群。在 1163438 名患有免疫介导的炎症性疾病的成年人中,19119 人(1.6%)接受了靶向免疫调节治疗,181694 人(15.6%)接受了标准全身治疗。与普通人群相比,在对混杂因素(年龄、性别、贫困程度和吸烟状况)进行调整后,患有免疫介导的炎症性疾病的成年人发生 COVID-19 相关死亡的风险增加(HR 1.23,95%CI 1.20 - 1.27),在进一步对中介因素(体重指数[BMI]、心血管疾病、糖尿病和当前糖皮质激素使用情况)进行调整后(1.15,1.11 - 1.18)。患有免疫介导的炎症性疾病的成年人发生 COVID-19 相关重症监护入院或死亡的风险也增加(混杂因素调整后的 HR 1.24,95%CI 1.21 - 1.28;中介因素调整后的 1.16,1.12 - 1.19)以及住院风险(混杂因素调整后的 1.32,1.29 - 1.35;中介因素调整后的 1.20,1.17 - 1.23)。在事后分析中,免疫介导的炎症性疾病患者中,非白人种族群体发生重症 COVID-19 结局的风险高于白人种族群体(普通人群中也是如此)。在对混杂因素(年龄、性别、贫困程度、BMI、免疫介导的炎症性疾病[肠道、关节和皮肤]、心血管疾病、癌症[不包括非黑色素瘤皮肤癌]、中风和糖尿病)进行调整后,我们没有发现与使用标准全身治疗的患者相比,接受靶向治疗的成年人发生 COVID-19 相关死亡风险增加的证据(HR 1.03,95%CI 0.80 - 1.33),在额外对当前糖皮质激素使用情况进行调整后(1.01,0.78 - 1.30)。与使用标准全身治疗的患者相比,使用肿瘤坏死因子抑制剂、白细胞介素(IL)-12/IL-23 抑制剂、IL-17 抑制剂、IL-6 抑制剂或 Janus 激酶抑制剂的成年人没有发生 COVID-19 相关死亡风险增加的证据。利妥昔单抗与 COVID-19 相关死亡风险增加相关(HR 1.68,95%CI 1.11 - 2.56),在排除血液系统恶性肿瘤或器官移植患者后有所减弱(1·· - ·)。
免疫介导的炎症性疾病患者的 COVID-19 死亡和住院率更高。与使用标准全身治疗相比,并在对混杂因素(年龄、性别、贫困程度、BMI、免疫介导的炎症性疾病[肠道、关节和皮肤]、心血管疾病、癌症[不包括非黑色素瘤皮肤癌]、中风和糖尿病)进行调整后,我们没有发现大多数用于免疫介导的炎症性疾病的靶向免疫调节药物使用者发生不良 COVID-19 结局的风险增加。
英国医学研究理事会、伦敦国王学院和盖伊与圣托马斯国民保健服务基金会信托基金的 NIHR 生物医学研究中心以及惠康信托基金会。