Department of Non-Communicable Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Department of Non-Communicable Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Lancet. 2021 May 8;397(10286):1711-1724. doi: 10.1016/S0140-6736(21)00634-6. Epub 2021 Apr 30.
COVID-19 has disproportionately affected minority ethnic populations in the UK. Our aim was to quantify ethnic differences in SARS-CoV-2 infection and COVID-19 outcomes during the first and second waves of the COVID-19 pandemic in England.
We conducted an observational cohort study of adults (aged ≥18 years) registered with primary care practices in England for whom electronic health records were available through the OpenSAFELY platform, and who had at least 1 year of continuous registration at the start of each study period (Feb 1 to Aug 3, 2020 [wave 1], and Sept 1 to Dec 31, 2020 [wave 2]). Individual-level primary care data were linked to data from other sources on the outcomes of interest: SARS-CoV-2 testing and positive test results and COVID-19-related hospital admissions, intensive care unit (ICU) admissions, and death. The exposure was self-reported ethnicity as captured on the primary care record, grouped into five high-level census categories (White, South Asian, Black, other, and mixed) and 16 subcategories across these five categories, as well as an unknown ethnicity category. We used multivariable Cox regression to examine ethnic differences in the outcomes of interest. Models were adjusted for age, sex, deprivation, clinical factors and comorbidities, and household size, with stratification by geographical region.
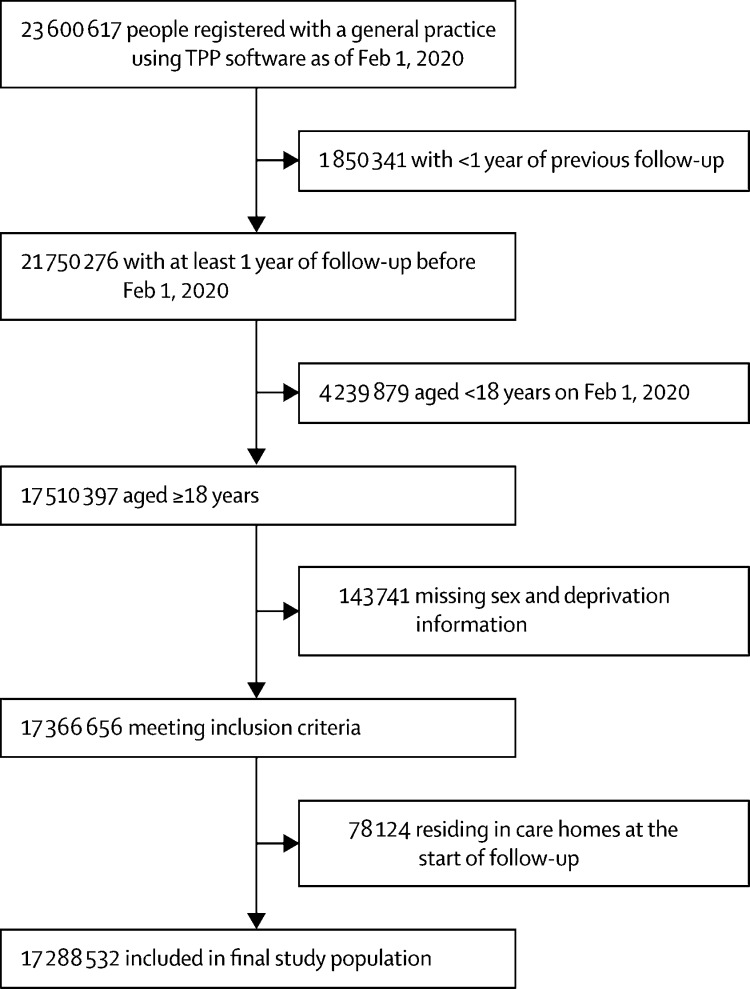
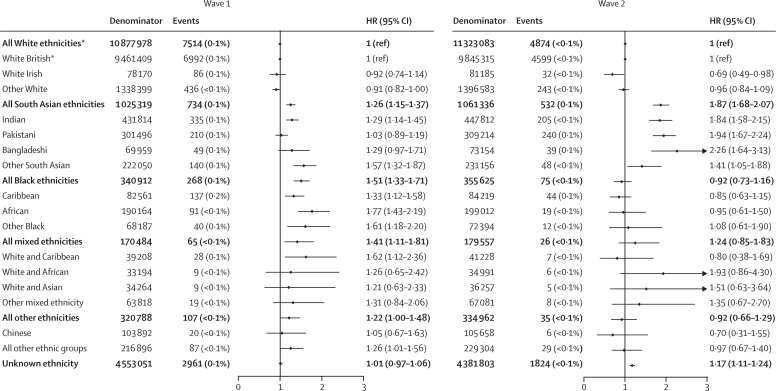
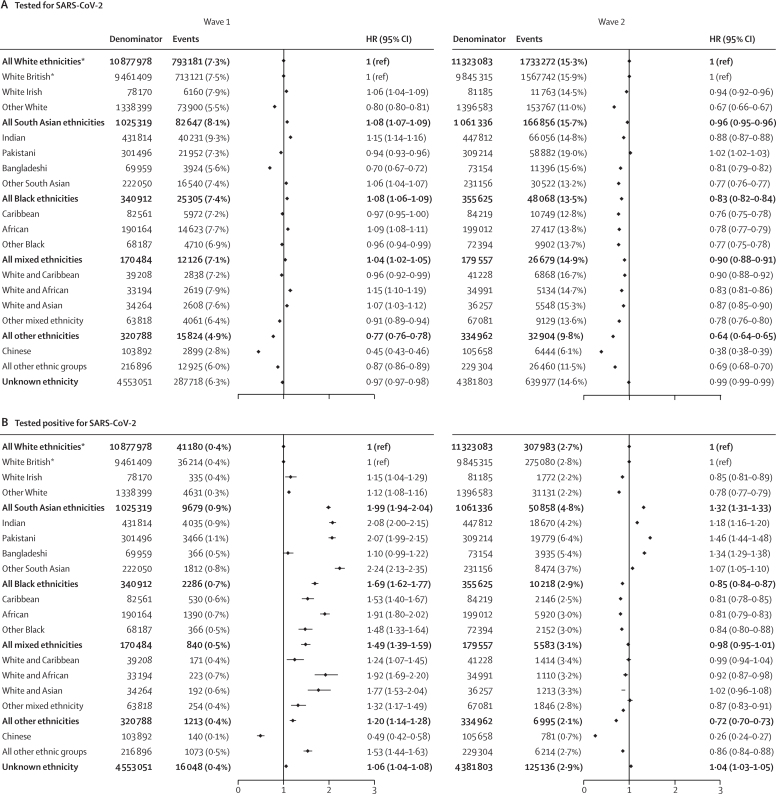
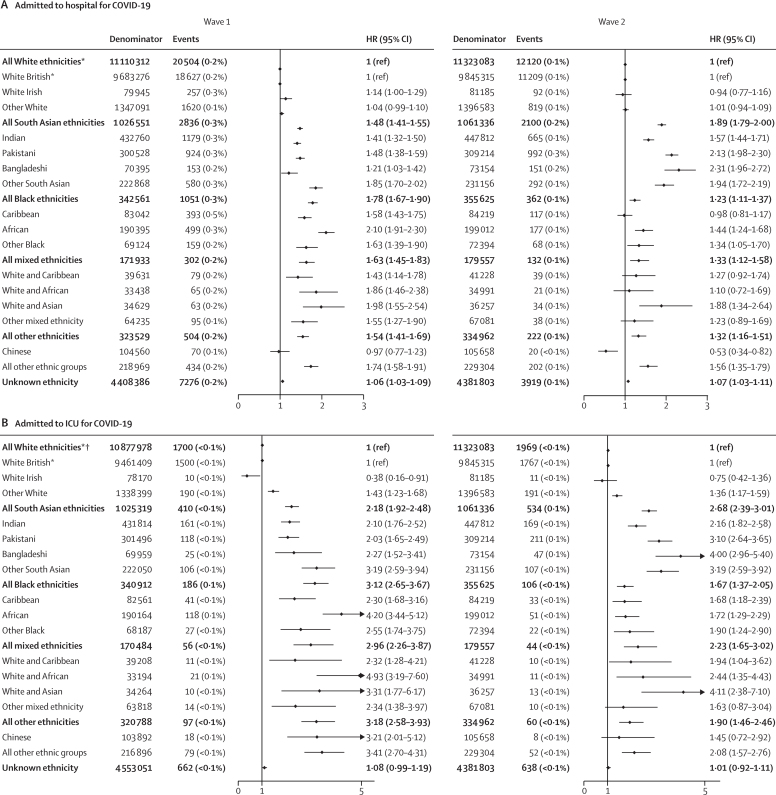
Of 17 288 532 adults included in the study (excluding care home residents), 10 877 978 (62·9%) were White, 1 025 319 (5·9%) were South Asian, 340 912 (2·0%) were Black, 170 484 (1·0%) were of mixed ethnicity, 320 788 (1·9%) were of other ethnicity, and 4 553 051 (26·3%) were of unknown ethnicity. In wave 1, the likelihood of being tested for SARS-CoV-2 infection was slightly higher in the South Asian group (adjusted hazard ratio 1·08 [95% CI 1·07-1·09]), Black group (1·08 [1·06-1·09]), and mixed ethnicity group (1·04 [1·02-1·05]) and was decreased in the other ethnicity group (0·77 [0·76-0·78]) relative to the White group. The risk of testing positive for SARS-CoV-2 infection was higher in the South Asian group (1·99 [1·94-2·04]), Black group (1·69 [1·62-1·77]), mixed ethnicity group (1·49 [1·39-1·59]), and other ethnicity group (1·20 [1·14-1·28]). Compared with the White group, the four remaining high-level ethnic groups had an increased risk of COVID-19-related hospitalisation (South Asian group 1·48 [1·41-1·55], Black group 1·78 [1·67-1·90], mixed ethnicity group 1·63 [1·45-1·83], other ethnicity group 1·54 [1·41-1·69]), COVID-19-related ICU admission (2·18 [1·92-2·48], 3·12 [2·65-3·67], 2·96 [2·26-3·87], 3·18 [2·58-3·93]), and death (1·26 [1·15-1·37], 1·51 [1·31-1·71], 1·41 [1·11-1·81], 1·22 [1·00-1·48]). In wave 2, the risks of hospitalisation, ICU admission, and death relative to the White group were increased in the South Asian group but attenuated for the Black group compared with these risks in wave 1. Disaggregation into 16 ethnicity groups showed important heterogeneity within the five broader categories.
Some minority ethnic populations in England have excess risks of testing positive for SARS-CoV-2 and of adverse COVID-19 outcomes compared with the White population, even after accounting for differences in sociodemographic, clinical, and household characteristics. Causes are likely to be multifactorial, and delineating the exact mechanisms is crucial. Tackling ethnic inequalities will require action across many fronts, including reducing structural inequalities, addressing barriers to equitable care, and improving uptake of testing and vaccination.
Medical Research Council.
新冠疫情在英国对少数族裔人群造成了不成比例的影响。我们的目的是量化在英格兰 COVID-19 大流行的第一波和第二波期间,SARS-CoV-2 感染和 COVID-19 结局在不同族裔之间的差异。
我们对在英格兰注册的成年人(年龄≥18 岁)进行了一项观察性队列研究,这些成年人的电子健康记录可通过 OpenSAFELY 平台获得,并且在每个研究期间(2020 年 2 月 1 日至 8 月 3 日[第一波]和 2020 年 9 月 1 日至 12 月 31 日[第二波])开始前至少有 1 年的连续注册。将初级保健数据与其他来源的数据进行关联,以了解与 SARS-CoV-2 检测和阳性检测结果以及 COVID-19 相关的住院、重症监护病房(ICU)入院和死亡等结果。暴露因素是初级保健记录中记录的自我报告的族裔,分为五个高一级普查类别(白人、南亚裔、黑人、其他和混合)和这五个类别中的 16 个子类别,以及一个未知族裔类别。我们使用多变量 Cox 回归来研究感兴趣的结果之间的族裔差异。这些模型调整了年龄、性别、贫困程度、临床因素和合并症以及家庭规模,并按地理位置进行分层。
在纳入的 17288532 名成年人中(不包括养老院居民),10877978 名(62.9%)为白人,1025319 名(5.9%)为南亚裔,340912 名(2.0%)为黑人,170484 名(1.0%)为混合族裔,320788 名(1.9%)为其他族裔,4553051 名(26.3%)为未知族裔。在第一波中,南亚裔(调整后的危险比 1.08[95%CI 1.07-1.09])、黑人(1.08[1.06-1.09])和混合族裔(1.04[1.02-1.05])群体接受 SARS-CoV-2 感染检测的可能性略高,而其他族裔(0.77[0.76-0.78])群体接受 SARS-CoV-2 感染检测的可能性较低。南亚裔(1.99[1.94-2.04])、黑人(1.69[1.62-1.77])、混合族裔(1.49[1.39-1.59])和其他族裔(1.20[1.14-1.28])群体检测呈 SARS-CoV-2 阳性的风险更高。与白人相比,其余四个高一级族裔群体的 COVID-19 相关住院风险增加(南亚裔 1.48[1.41-1.55],黑人 1.78[1.67-1.90],混合族裔 1.63[1.45-1.83],其他族裔 1.54[1.41-1.69]),COVID-19 相关 ICU 入院风险增加(2.18[1.92-2.48],3.12[2.65-3.67],2.96[2.26-3.87],3.18[2.58-3.93])和死亡风险增加(1.26[1.15-1.37],1.51[1.31-1.71],1.41[1.11-1.81],1.22[1.00-1.48])。在第二波中,与白人相比,南亚裔群体的住院、ICU 入院和死亡风险增加,但与第一波相比,黑人群体的这些风险有所减弱。将人群分为 16 个族裔群体显示出五个更广泛类别内部存在重要的异质性。
英格兰的一些少数族裔人群与白人相比,SARS-CoV-2 检测呈阳性和 COVID-19 结局不良的风险更高,即使在考虑了社会人口学、临床和家庭特征方面的差异后也是如此。原因可能是多方面的,明确确切的机制至关重要。解决族裔不平等问题需要在许多方面采取行动,包括减少结构性不平等、解决公平护理方面的障碍以及提高检测和疫苗接种的接受率。
医学研究理事会。