Atrium Health Neurosciences Institute, Carolinas Medical Center, University of North Carolina School of Medicine-Charlotte Campus, Charlotte, North Carolina, United States of America.
Lewis Katz School of Medicine, Temple University, Philadelphia, Pennsylvania, United States of America.
PLoS One. 2022 Jun 14;17(6):e0258614. doi: 10.1371/journal.pone.0258614. eCollection 2022.
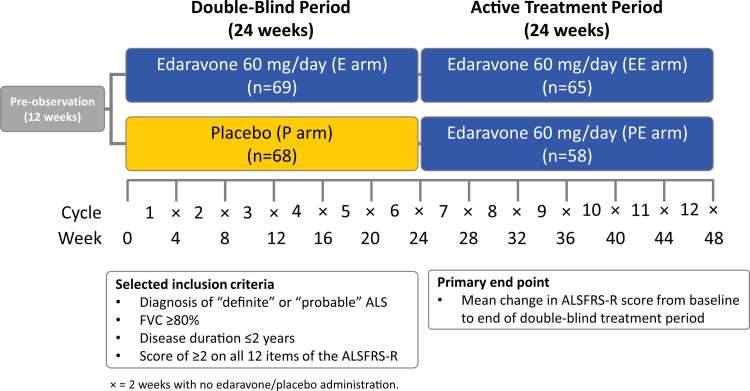
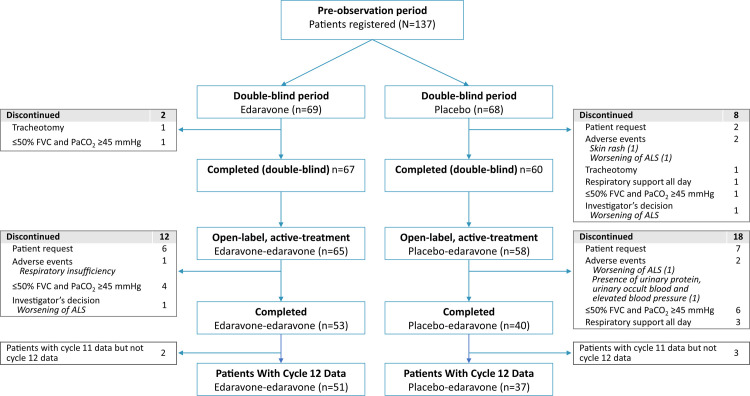
Edaravone slowed the rate of functional decline in subjects with amyotrophic lateral sclerosis (ALS) in phase 3 study MCI186-19 (Study 19). One of the Study 19 inclusion criteria was forced vital capacity (FVC) ≥80% of predicted (≥80%p). Therefore, the study provided no information on edaravone efficacy in subjects with FVC <80%p. In Study 19, 24-week, double-blind treatment was followed by open-label treatment where all subjects received edaravone. At 24 weeks, some subjects had FVC <80%p (FVC24 <80%p). This allowed for post-hoc assessment of the effects of edaravone in subgroups of subjects with FVC24 ≥80%p vs <80%p.
To address the question of the efficacy of edaravone in ALS patients with FVC <80%p.
Post-hoc analysis of Study 19 comparing edaravone efficacy at week 48 in subjects with FVC24 ≥80%p vs <80%p.
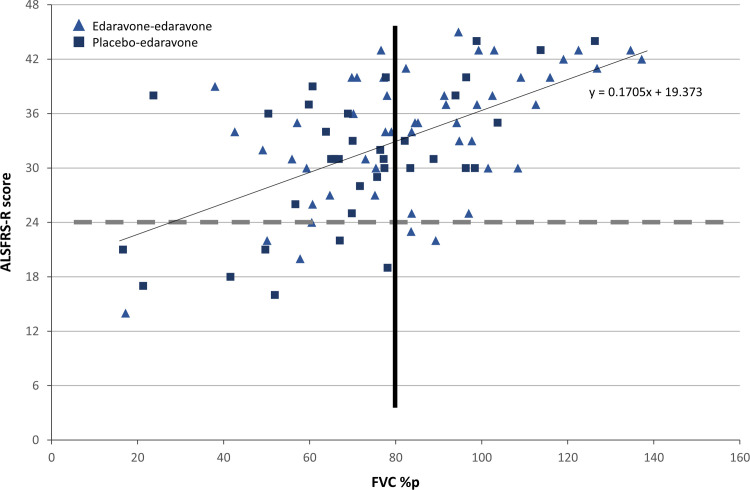
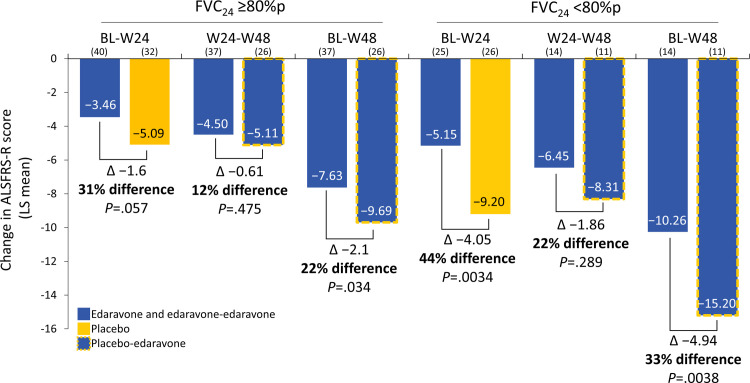
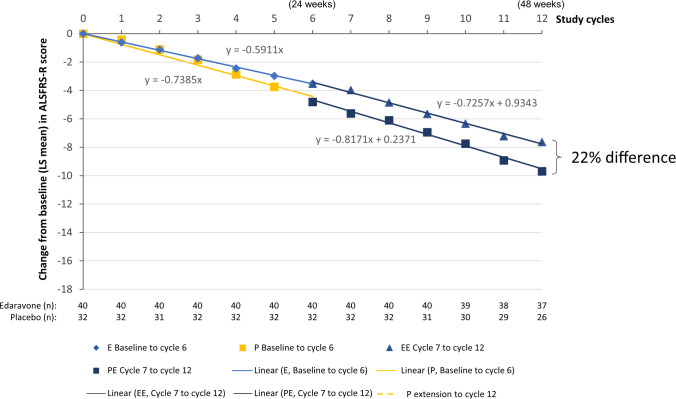
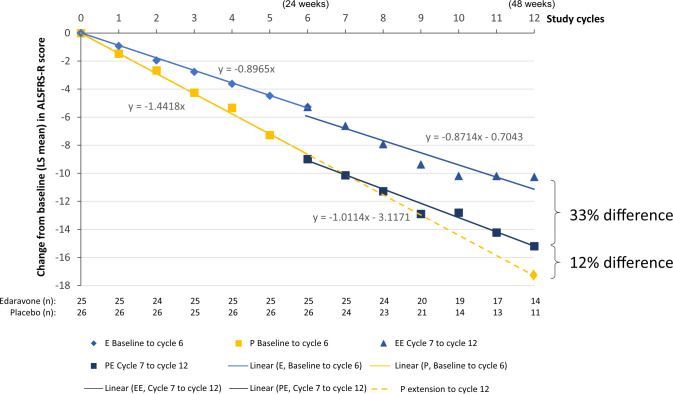
With edaravone treatment, subjects in both the FVC24 ≥80%p and the FVC24 <80%p subgroups experienced a reduction in ALS Functional Rating Scale-Revised (ALSFRS-R) score loss vs placebo subjects through week 48. For the FVC24 ≥80%p subgroup, the changes in ALSFRS-R scores from baseline to week 48 were -7.63 for edaravone-edaravone vs -9.69 for placebo-edaravone, a difference of 2.05 (P = .034; 95% CI: 0.16, 3.94). For the FVC24 <80%p subgroup, the changes in ALSFRS-R scores from baseline to week 48 were -10.26 for edaravone-edaravone vs -15.20 for placebo-edaravone, a difference of 4.94 (P = .0038; 95% CI: 1.64, 8.25). Linear regression analysis indicated that, in the FVC24 <80%p subgroup, there was a notable change in the slope of the ALSFRS-R score-vs-time graph after the start of edaravone treatment.
ALS subjects in the Study 19 placebo arm had a slowing in disease progression, even when edaravone was added with an FVC of <80%p prior to starting edaravone. A randomized, placebo-controlled study is needed to validate these post-hoc findings.
依达拉奉在 3 期研究 MCI186-19(研究 19)中减缓了肌萎缩侧索硬化症(ALS)患者的功能下降速度。研究 19 的纳入标准之一是用力肺活量(FVC)≥预测值的 80%(≥80%p)。因此,该研究没有提供依达拉奉在 FVC <80%p 的患者中的疗效信息。在研究 19 中,24 周的双盲治疗后进行开放标签治疗,所有患者均接受依达拉奉治疗。在 24 周时,一些患者的 FVC <80%p(FVC24 <80%p)。这使得可以对 FVC24 ≥80%p 和 <80%p 的患者亚组进行依达拉奉疗效的事后评估。
解决 FVC <80%p 的 ALS 患者中依达拉奉疗效的问题。
对研究 19 进行事后分析,比较 FVC24 ≥80%p 和 <80%p 的患者在第 48 周时依达拉奉的疗效。
在依达拉奉治疗下,FVC24 ≥80%p 和 FVC24 <80%p 亚组的患者在第 48 周时通过安慰剂治疗的 ALS 功能评定量表修订版(ALSFRS-R)评分损失均减少。对于 FVC24 ≥80%p 亚组,从基线到第 48 周的 ALSFRS-R 评分变化为依达拉奉-依达拉奉组为-7.63,安慰剂-依达拉奉组为-9.69,差异为 2.05(P=.034;95%CI:0.16,3.94)。对于 FVC24 <80%p 亚组,从基线到第 48 周的 ALSFRS-R 评分变化为依达拉奉-依达拉奉组为-10.26,安慰剂-依达拉奉组为-15.20,差异为 4.94(P=.0038;95%CI:1.64,8.25)。线性回归分析表明,在 FVC24 <80%p 亚组中,依达拉奉治疗开始后,ALSFRS-R 评分与时间关系图的斜率明显发生变化。
即使在开始依达拉奉治疗前 FVC <80%p 时添加依达拉奉,研究 19 安慰剂组的 ALS 患者的疾病进展也有所减缓。需要进行随机、安慰剂对照研究来验证这些事后发现。