Gonzalez Noah, Lucas Jean-Marc P, Winegar Austin, Den Haese Jason, Danahy Paul
College of Osteopathic Medicine, Lake Erie College of Osteopathic Medicine, Erie, USA.
College of Osteopathic Medicine, Lake Erie College of Osteopathic Medicine, Bradenton, USA.
Cureus. 2022 May 12;14(5):e24943. doi: 10.7759/cureus.24943. eCollection 2022 May.
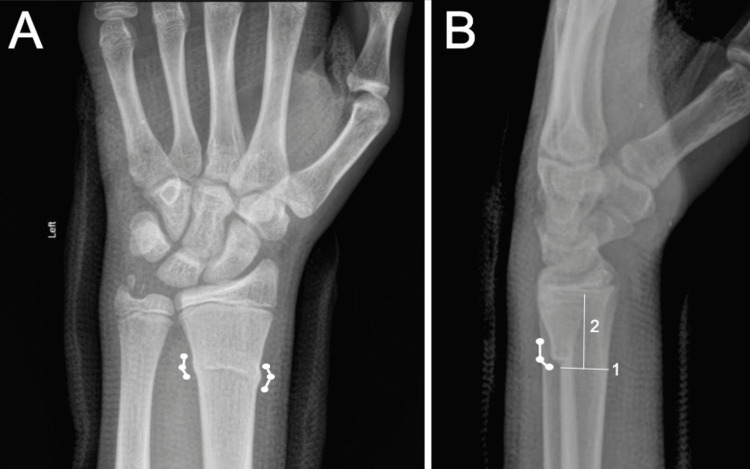
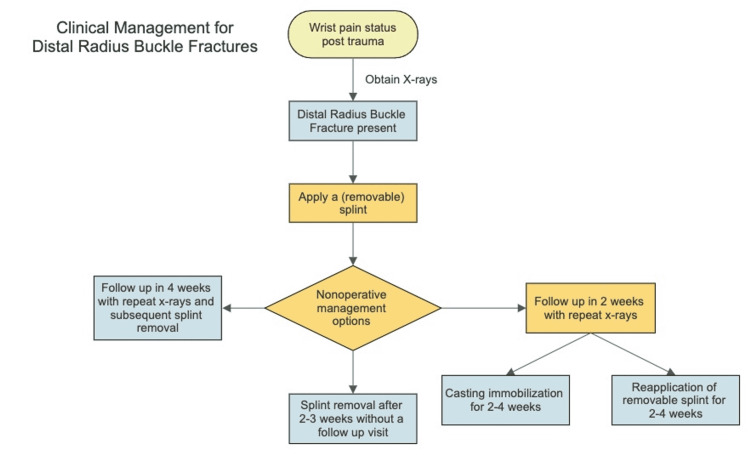
Distal radius buckle fractures (DRBFs) are the most common pediatric fractures and resemble the rounded portion of a Greek pillar or torus. They result from compressive forces applied to a child's highly plastic radius. DRBFs lack cortical and physeal disruption, which makes them relatively stable. In this review, we discuss angled DRBFs, a hypothesized subset of buckle fractures that results from an off-center compressive force. Some authors refute the existence of angled DRBFs, instead proposing new criteria for DRBF classification: measuring more than 1 cm away from the physis with two to three inflection points. Without universal diagnostic criteria, misdiagnosis is common, and the utilization of flexible treatment modalities is infrequent. Rigid immobilization with short-arm casting continues to be the mainstay of treatment in clinical practice. Yet, new protocols implementing removable elastic bandages have had comparable results to casting, including reduced healthcare expenditure, less stiffness, and improved convenience and patient tolerability. Despite the discrepancies in categorizing DRBFs, complication rates remain low, and diagnostic confusion insignificantly affects clinical outcomes. Angled DRBFs have been theorized to have intraphyseal extension, making them unstable Salter-Harris fractures. Radiographic evidence supporting or denying this claim is limited. Further research is essential to determine the stability of the angled DRBF subtype and whether they should continue to be defined and managed as buckle fractures.
桡骨远端青枝骨折(DRBFs)是最常见的儿童骨折,形似希腊立柱或圆环的圆形部分。它们是由于作用于儿童可塑性很强的桡骨的压缩力所致。DRBFs没有皮质和骨骺损伤,这使其相对稳定。在本综述中,我们讨论斜形DRBFs,这是一种推测的青枝骨折亚型,由偏心压缩力导致。一些作者驳斥斜形DRBFs的存在,而是提出了DRBF分类的新标准:距骨骺超过1厘米,有两到三个拐点。由于没有通用的诊断标准,误诊很常见,而且很少使用灵活的治疗方式。临床实践中,短臂石膏固定仍然是主要的治疗方法。然而,采用可拆除弹性绷带的新方案与石膏固定效果相当,包括降低医疗费用、减少僵硬程度以及提高便利性和患者耐受性。尽管在DRBFs分类上存在差异,但并发症发生率仍然很低,诊断混淆对临床结果的影响微不足道。理论上,斜形DRBFs有骨骺内延伸,使其成为不稳定的Salter-Harris骨折。支持或否定这一说法的影像学证据有限。进一步的研究对于确定斜形DRBFs亚型的稳定性以及它们是否应继续被定义为青枝骨折并按此处理至关重要。