Meidan Talia G, Lanfear Allison T, Squiers John J, Hamandi Mohanad, Lytle Bruce W, DiMaio J Michael, Smith Robert L
Baylor Scott & White Research Institute, Baylor Scott & White The Heart Hospital - Plano, Plano, Tex.
Department of Cardiothoracic Surgery, Baylor Scott & White The Heart Hospital - Plano, Plano, Tex.
JTCVS Tech. 2022 Feb 24;13:46-51. doi: 10.1016/j.xjtc.2022.01.023. eCollection 2022 Jun.
Despite the recent increase in the use of minimally invasive approaches to mitral valve surgery in patients with a prior sternotomy, the outcomes of the robotic approach to mitral valve surgery in this patient population have not been examined.
We retrospectively reviewed 342 consecutive patients who underwent mitral valve surgery after a prior sternotomy between 2013 and 2020, in which the robotic approach was used in 21 patients (6.1%). We reviewed the clinical details of these 21 patients.
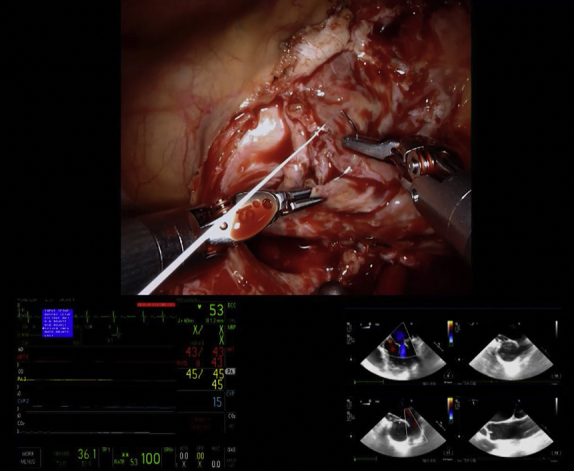
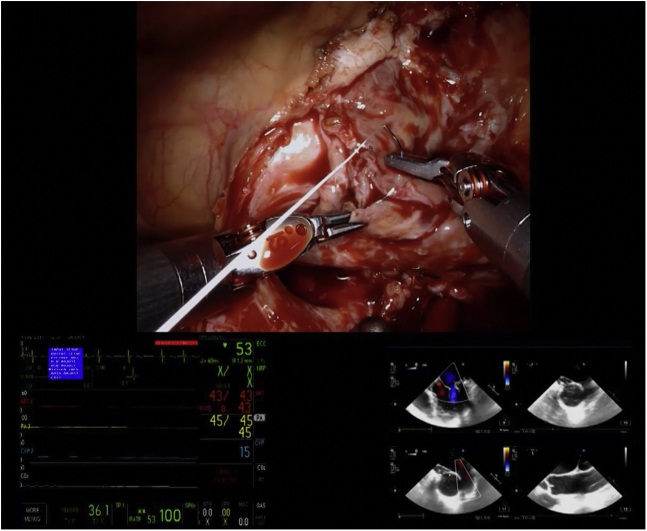
The median age was 71 years [interquartile range 64.00, 74.00 years], and mean Society of Thoracic Surgeons Predicted Risk of Mortality was 4.2% ± 3.8%. The indication for mitral valve surgery was degenerative mitral valve disease in 33.3% (7/21), functional disease in 28.6% (6/21), mixed disease in 4.8% (1/21), rheumatic disease in 9.5% (2/21), and failed repair for degenerative disease in 23.8% (5/21). No cases required conversion from robotic assistance to alternative approaches, there were no intraoperative deaths, and intraoperative transesophageal echocardiogram confirmed complete elimination of mitral regurgitation in 90.5% (19/21) of cases. Thirty-day mortality was 0.0% (0/21), and 1-year mortality was 4.8% (1/21). There were no strokes or wound infections at 30 days, and 14.3% (3/21) of patients received intraoperative blood product transfusions.
The results of this retrospective review suggest that the robotic approach to mitral valve surgery in patients with a prior sternotomy is safe in experienced hands. Although some centers have considered prior sternotomy a relative contraindication to robotic mitral valve surgery, this approach is feasible and can be considered an option for experienced surgeons.
尽管近期先前接受过胸骨切开术的患者在二尖瓣手术中采用微创方法的情况有所增加,但该患者群体中机器人二尖瓣手术的结果尚未得到研究。
我们回顾性分析了2013年至2020年间342例先前接受过胸骨切开术且随后接受二尖瓣手术的连续患者,其中21例(6.1%)采用了机器人手术方法。我们回顾了这21例患者的临床细节。
患者年龄中位数为71岁[四分位间距64.00,74.00岁],胸外科医师协会预测的平均死亡风险为4.2%±3.8%。二尖瓣手术的适应证为退行性二尖瓣疾病33.3%(7/21)、功能性疾病28.6%(6/21)、混合性疾病4.8%(1/21)、风湿性疾病9.5%(2/21)以及退行性疾病修复失败23.8%(5/21)。无一例需要从机器人辅助转换为其他手术方法,无术中死亡,术中经食管超声心动图证实90.5%(19/21)的病例二尖瓣反流完全消除。30天死亡率为0.0%(0/21),1年死亡率为4.8%(1/21)。30天时无中风或伤口感染,14.3%(3/21)的患者术中接受了血液制品输血。
这项回顾性研究结果表明,在经验丰富的术者手中,先前接受过胸骨切开术的患者采用机器人二尖瓣手术是安全的。尽管一些中心认为先前的胸骨切开术是机器人二尖瓣手术的相对禁忌证,但这种方法是可行的,并且可以被经验丰富的外科医生视为一种选择。