Chen Xiaofeng, Li Wei, Wu Xiaofeng, Zhao Fengjiao, Wang Deqiang, Wu Hao, Gu Yanhong, Li Xiao, Qian Xiaofeng, Hu Jun, Li Changxian, Xia Yongxiang, Rao Jianhua, Dai Xinzheng, Shao Qianwen, Tang Jie, Li Xiangcheng, Shu Yongqian
Department of Oncology, Jiangsu Province Hospital, The First Affiliated Hospital, Nanjing Medical University, Nanjing, China.
Department of Oncology, Pukou Branch of Jiangsu People's Hospital, Nanjing, China.
Front Oncol. 2022 May 31;12:909035. doi: 10.3389/fonc.2022.909035. eCollection 2022.
Immune checkpoint inhibitors plus antiangiogenic tyrosine kinase inhibitors may offer a first-line treatment for advanced hepatocellular carcinoma (HCC). In this phase 2 trial [registered with clinicaltrials.gov (NCT04052152)], we investigated the safety and efficacy of first-line anti-PD-1 antibody sintilimab plus antiangiogenic TKI anlotinib for advanced HCC.
Pathologically-proven advanced HCC patients received sintilimab (200 mg) on day 1 and anlotinib (12 mg) once daily on days 1 to 14 every 3 weeks, with a safety run-in for the first six participants to assess dose-limiting toxicities (DLTs). The primary endpoints were safety and objective response rate (ORR) per RECIST v1.1.
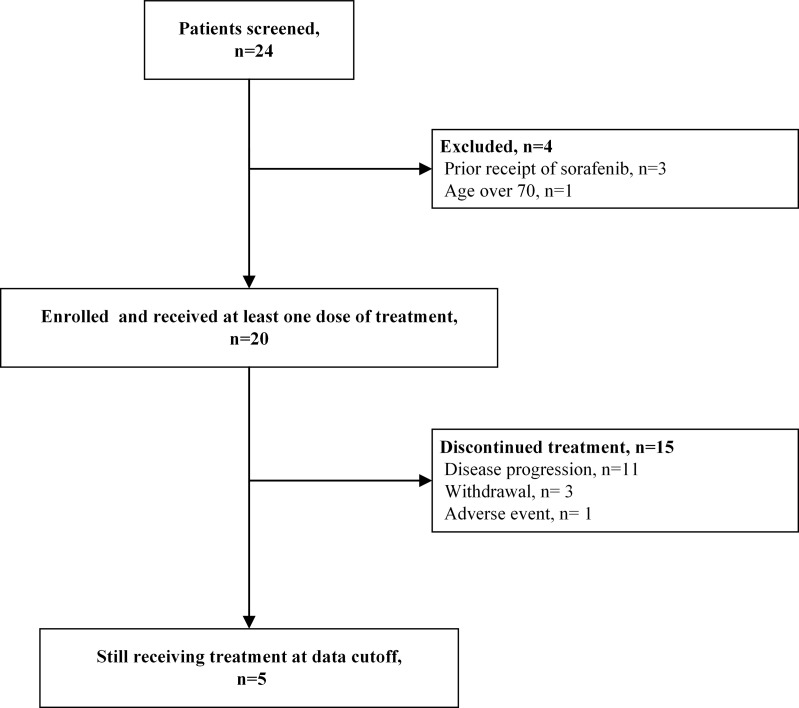
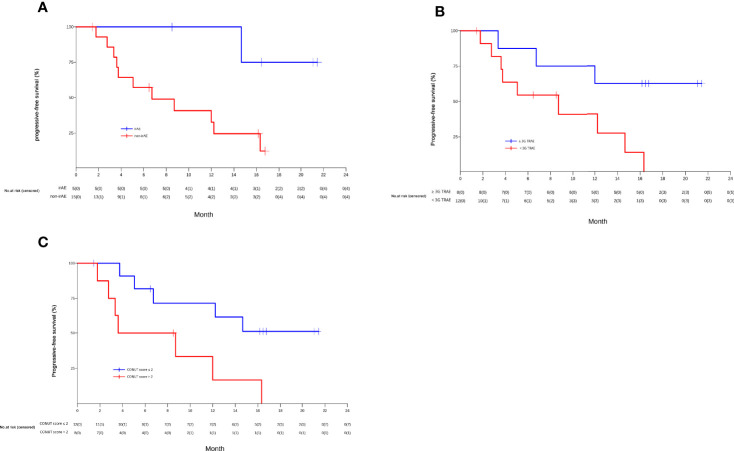
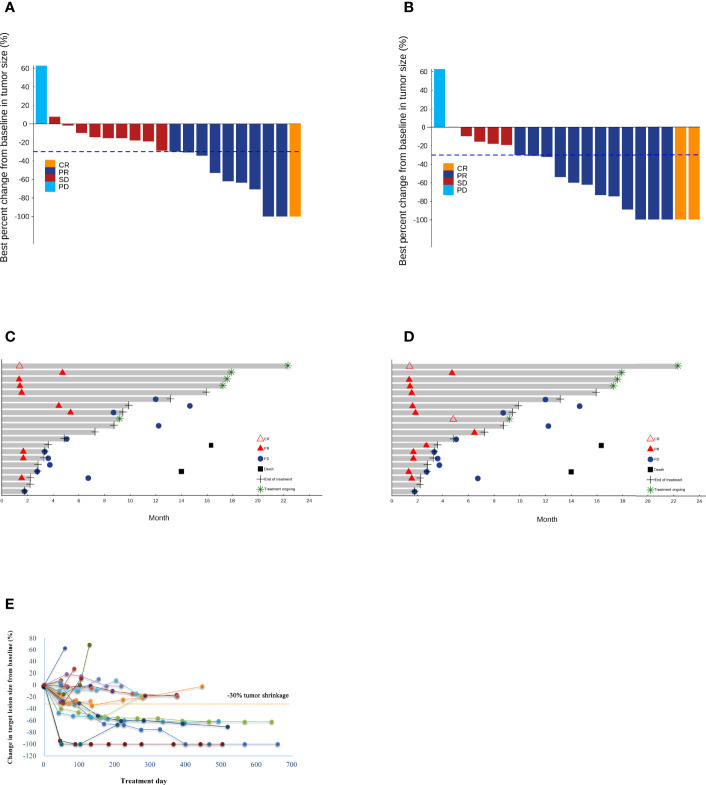
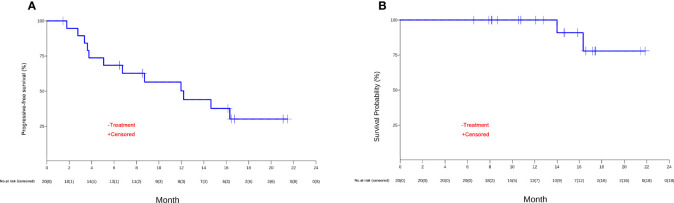
Twenty advanced HCC patients were enrolled. No DLTs occurred in the safety run-in. All patients had treatment-related adverse events (TRAEs). Grade 3 TRAEs occurred in 8 (40.0%) patients, the most common being decreased platelet count (10.0%) and increased γ-glutamyl transferase (10.0%). No grade 4/5 TRAEs occurred. Five (25%) patients developed immune-related AEs. The ORR was 35.0% (95%CI 15.4%-59.2%) per RECIST v1.1 and 55.0% (95%CI 31.5%-76.9%) per modified RECIST. At data cutoff (March 31, 2021), the median progression-free survival was 12.2 months (95%CI, 3.8 to not reached). The median PFS was significantly longer in patients with lower LDH levels (not reached [NR], 95% CI, 8.7 to NR vs. higher LDH levels 5.2 months, 95% CI 3.4 to NR; =0.020) and a CONUT score ≤2 (NR, 95% CI 5.1 to NR vs. CONUT score >2 6.2 months, 95% CI 1.8 to NR; =0.020). Furthermore, patients showing tumor response had a significantly higher median proportion of CD16CD56 NK cells than patients who had stable or progressive disease (21.6% vs. 14.6%; P=0.026).
Sintilimab plus anlotinib showed promising clinical activities with manageable toxicity as first-line treatment of advanced HCC.
免疫检查点抑制剂联合抗血管生成酪氨酸激酶抑制剂可能为晚期肝细胞癌(HCC)提供一线治疗方案。在这项2期试验[已在clinicaltrials.gov(NCT04052152)注册]中,我们研究了一线抗PD-1抗体信迪利单抗联合抗血管生成酪氨酸激酶抑制剂安罗替尼治疗晚期HCC的安全性和疗效。
经病理证实的晚期HCC患者在第1天接受信迪利单抗(200mg)治疗,安罗替尼(12mg)在第1至14天每天一次,每3周重复一次,前6名参与者进行安全性导入期以评估剂量限制性毒性(DLT)。主要终点是根据RECIST v1.1标准评估的安全性和客观缓解率(ORR)。
入组20例晚期HCC患者。安全性导入期未发生DLT。所有患者均发生治疗相关不良事件(TRAE)。3级TRAE发生在8例(40.0%)患者中,最常见的是血小板计数降低(10.0%)和γ-谷氨酰转移酶升高(10.0%)。未发生4/5级TRAE。5例(25%)患者发生免疫相关AE。根据RECIST v1.1标准,ORR为35.0%(95%CI 15.4%-59.2%),根据改良RECIST标准为55.0%(95%CI 31.5%-76.9%)。在数据截止时(2021年3月31日),中位无进展生存期为12.2个月(95%CI,3.8至未达到)。乳酸脱氢酶(LDH)水平较低的患者中位无进展生存期显著更长(未达到[NR],95%CI,8.7至未达到,与LDH水平较高的患者5.2个月,95%CI 3.4至未达到;P=0.020),且CONUT评分≤(2NR,95%CI 5.1至未达到,与CONUT评分>2的患者6.2个月,95%CI 1.8至未达到;P=0.020)。此外,显示肿瘤缓解的患者CD16CD56自然杀伤细胞的中位比例显著高于疾病稳定或进展的患者(21.6%对14.6%;P=0.026)。
信迪利单抗联合安罗替尼作为晚期HCC的一线治疗方案显示出有前景的临床活性且毒性可控。