Arce-Álvarez Alexis, Salazar-Ardiles Camila, Cornejo Carlos, Paez Valeria, Vásquez-Muñoz Manuel, Stillner-Vilches Katherine, Jara Catherine R, Ramirez-Campillo Rodrigo, Izquierdo Mikel, Andrade David C
Exercise Applied Physiology Laboratory, Centro de Investigación en Fisiología y Medicina de Altura, Departamento Biomedico, Facultad de Ciencias de La Salud, Universidad de Antofagasta, Antofagasta, Chile.
Escuela de Kinesiología, Facultad de Salud, Universidad Católica Silva Henríquez, Santiago, Chile.
Front Physiol. 2022 Jun 6;13:894921. doi: 10.3389/fphys.2022.894921. eCollection 2022.
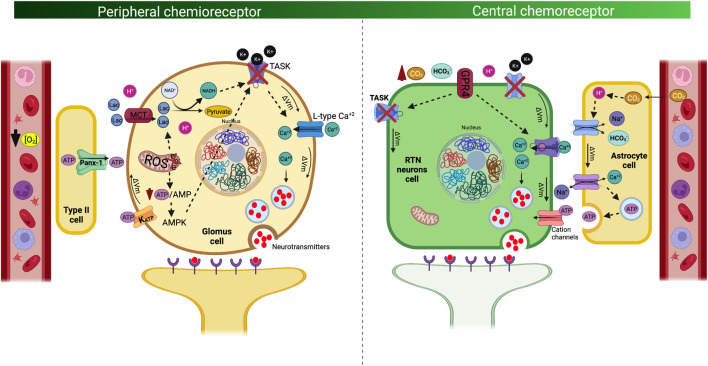
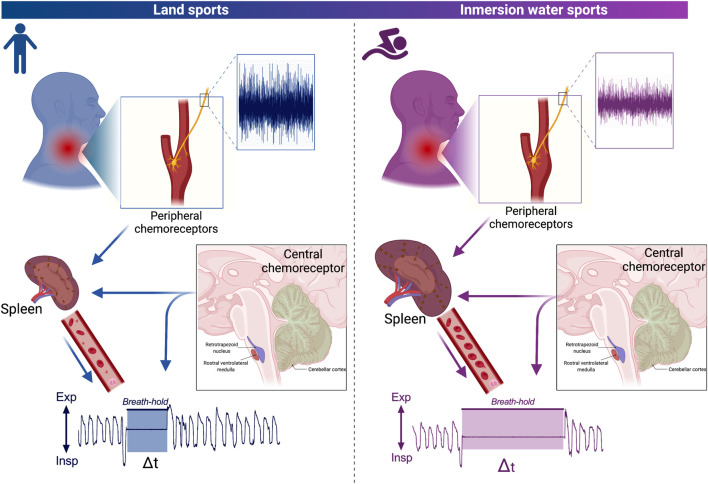
Immersion water sports involve long-term apneas; therefore, athletes must physiologically adapt to maintain muscle oxygenation, despite not performing pulmonary ventilation. Breath-holding (i.e., apnea) is common in water sports, and it involves a decrease and increases PaO and PaCO, respectively, as the primary signals that trigger the end of apnea. The principal physiological O sensors are the carotid bodies, which are able to detect arterial gases and metabolic alterations before reaching the brain, which aids in adjusting the cardiorespiratory system. Moreover, the principal H/CO sensor is the retrotrapezoid nucleus, which is located at the brainstem level; this mechanism contributes to detecting respiratory and metabolic acidosis. Although these sensors have been characterized in pathophysiological states, current evidence shows a possible role for these mechanisms as physiological sensors during voluntary apnea. Divers and swimmer athletes have been found to displayed longer apnea times than land sports athletes, as well as decreased peripheral O and central CO chemoreflex control. However, although chemosensitivity at rest could be decreased, we recently found marked sympathoexcitation during maximum voluntary apnea in young swimmers, which could activate the spleen (which is a reservoir organ for oxygenated blood). Therefore, it is possible that the chemoreflex, autonomic function, and storage/delivery oxygen organ(s) are linked to apnea in immersion water sports. In this review, we summarized the available evidence related to chemoreflex control in immersion water sports. Subsequently, we propose a possible physiological mechanistic model that could contribute to providing new avenues for understanding the respiratory physiology of water sports.
沉浸式水上运动涉及长时间的屏气;因此,运动员必须在生理上做出适应,以维持肌肉的氧合作用,尽管此时并未进行肺通气。憋气(即屏气)在水上运动中很常见,它分别涉及动脉血氧分压(PaO)降低和动脉血二氧化碳分压(PaCO)升高,这是触发屏气结束的主要信号。主要的生理氧传感器是颈动脉体,它能够在到达大脑之前检测动脉气体和代谢变化,这有助于调节心肺系统。此外,主要的氢离子/二氧化碳传感器是位于脑干水平的后梯形核;这种机制有助于检测呼吸性和代谢性酸中毒。尽管这些传感器已在病理生理状态下得到表征,但目前的证据表明,在自愿屏气期间,这些机制可能作为生理传感器发挥作用。潜水员和游泳运动员的屏气时间比陆上运动运动员更长,同时外周氧和中枢二氧化碳化学反射控制也有所降低。然而,尽管静息时的化学敏感性可能降低,但我们最近发现,年轻游泳运动员在最大自主屏气期间会出现明显的交感神经兴奋,这可能会激活脾脏(脾脏是含氧血液的储存器官)。因此,化学反射、自主神经功能以及储存/输送氧气的器官可能与沉浸式水上运动中的屏气有关。在这篇综述中,我们总结了与沉浸式水上运动中化学反射控制相关的现有证据。随后,我们提出了一个可能的生理机制模型,这可能有助于为理解水上运动的呼吸生理学提供新的途径。