Juliet Keidan Institute of Pediatric Gastroenterology Hepatology and Nutrition, Shaare Zedek Medical Center, Jerusalem, Israel.
The Faculty of Medicine, The Hebrew University of Jerusalem, Jerusalem, Israel.
Aliment Pharmacol Ther. 2022 Sep;56(5):794-801. doi: 10.1111/apt.17092. Epub 2022 Jun 23.
Patients enrolled in randomised controlled trials (RCTs) may differ from the target population due to restricted eligibility criteria.
To compare treatment response to biologics in routine practice for children with inflammatory bowel diseases (IBD) who would and would not have been eligible for enrolment in the regulatory RCT of the same drug.
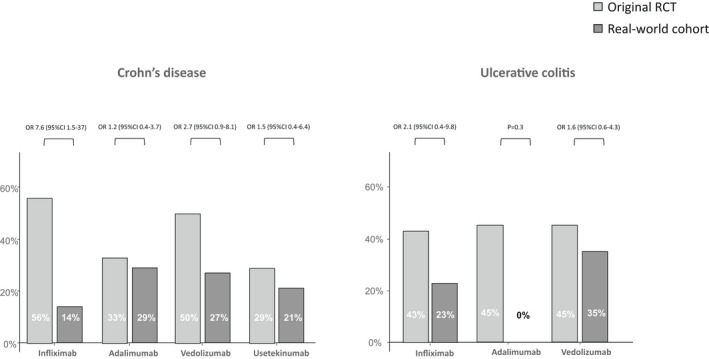
We enrolled children with IBD who initiated adalimumab, infliximab, vedolizumab or ustekinumab. The eligibility criteria as defined in the RCT of the corresponding biologic were applied to each patient. The primary outcome was 12-month steroid-free remission (SFR) without switching biologics or undergoing surgery.
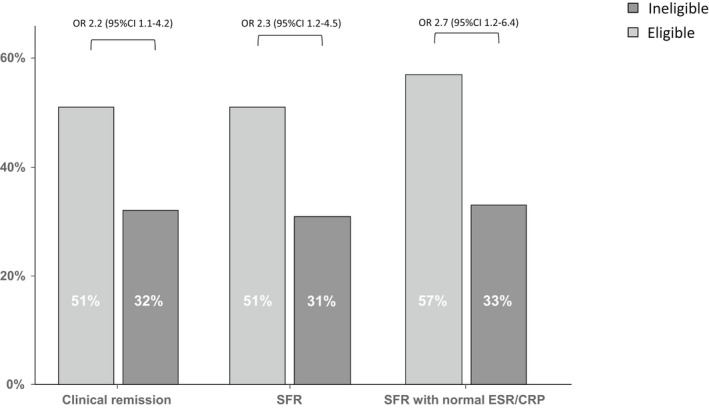
We screened 289 children (198 [68%] with Crohn's disease [CD], 91 [32%] with ulcerative colitis [UC]) with 326 initiations of biologics. Only 62 of 164 (38%) children with moderate-to-severe disease would have been eligible for inclusion in the original RCTs. The SFR rate was higher in the eligible children (51%) than in the ineligible children (31%; OR 2.3 [95%CI 1.2-4.5]; p = 0.01). The main exclusion criterion was prohibited previous therapies (47%). Ineligible CD patients were older, more often had a family history of IBD and had higher levels of CRP than eligible children; in UC there were no differences between the groups.
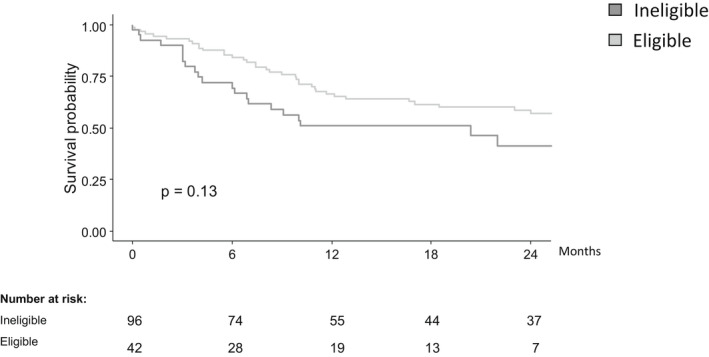
Most children with IBD who initiate biologics would not have been eligible to be included in the corresponding regulatory RCTs. The outcomes of ineligible patients were worse than for eligible patients. Results from RCTs should be interpreted with caution when applied to clinical practice.
由于入选标准受限,参加随机对照试验(RCT)的患者可能与目标人群不同。
比较生物制剂在常规治疗儿童炎症性肠病(IBD)中的治疗反应,这些儿童符合或不符合同一药物监管 RCT 的纳入标准。
我们纳入了开始接受阿达木单抗、英夫利昔单抗、维得利珠单抗或乌司奴单抗治疗的 IBD 儿童。每个患者均应用 RCT 中定义的纳入标准。主要结局是无激素治疗 12 个月缓解(SFR),不转换生物制剂或进行手术。
我们筛选了 289 名儿童(198 名[68%]患有克罗恩病[CD],91 名[32%]患有溃疡性结肠炎[UC]),其中 326 名儿童开始使用生物制剂。仅有 164 名中重度疾病儿童中的 62 名(38%)符合原始 RCT 的纳入标准。符合条件的儿童 SFR 率(51%)高于不符合条件的儿童(31%;OR 2.3 [95%CI 1.2-4.5];p=0.01)。主要排除标准是禁止使用既往治疗(47%)。不符合条件的 CD 患者年龄较大,更常伴有 IBD 家族史,且 CRP 水平高于符合条件的儿童;UC 组患儿之间无差异。
大多数开始使用生物制剂的 IBD 儿童不符合纳入相应监管 RCT 的标准。不符合条件的患者的结局比符合条件的患者差。在将 RCT 结果应用于临床实践时应谨慎解读。