Lozano-Edo Silvia, Roselló-Lletí Esther, Sánchez-Lázaro Ignacio, Tarazón Estefanía, Portolés Manuel, Ezzitouny Maryem, Lopez-Vilella Raquel, Arnau Miguel Angel, Almenar Luis, Martínez-Dolz Luis
Heart Failure and Transplantation Unit, Cardiology Department, University and Polytechnic La Fe Hospital, 46026 Valencia, Spain.
Clinical and Translational Research Group in Cardiology, Health Research Institute Hospital La Fe (IIS La Fe), 46026 Valencia, Spain.
J Pers Med. 2022 May 31;12(6):913. doi: 10.3390/jpm12060913.
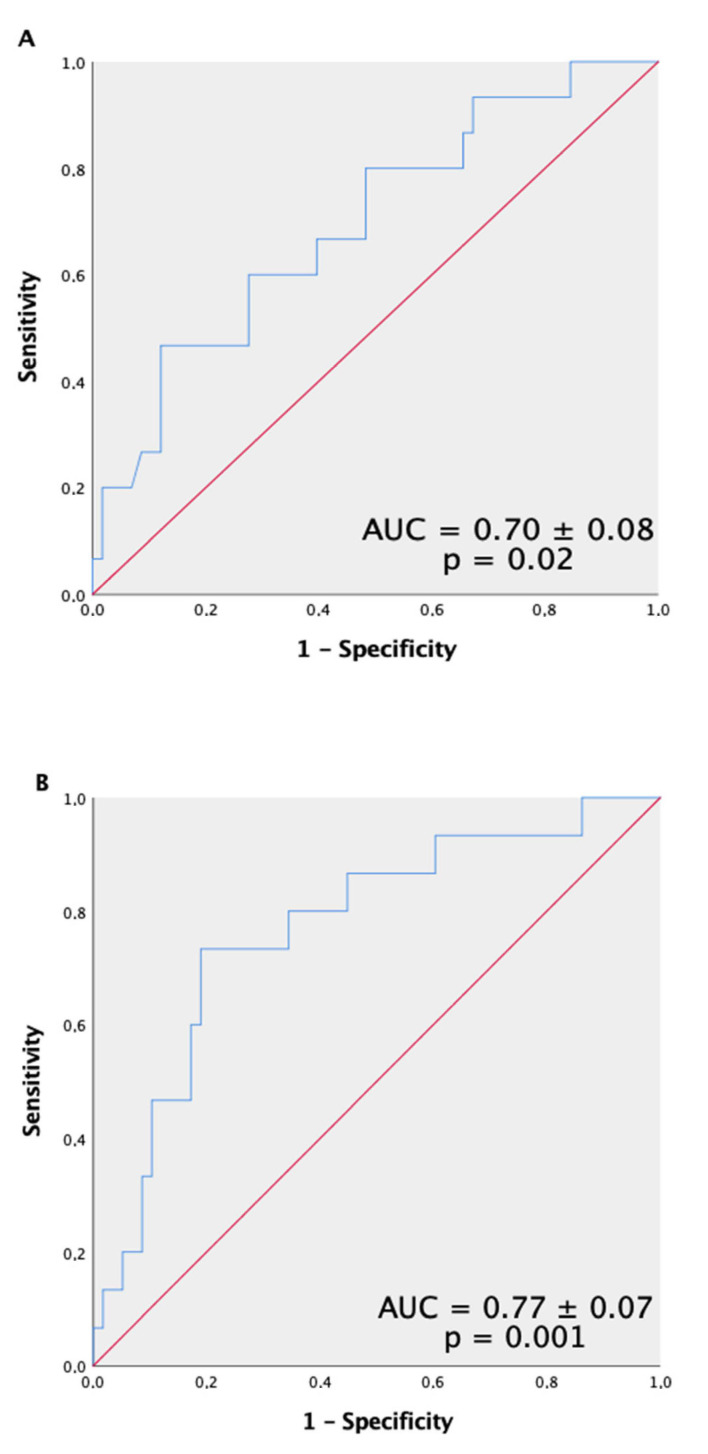
The non-invasive diagnosis of acute cellular rejection (ACR) is a major challenge. We performed a molecular study analyzing the predictive capacity of serum RanGTPase AP1 (RANGAP1) for diagnosing ACR during the first year after heart transplantation (HT). We included the serum samples of 75 consecutive HT patients, extracted after clinical stability, to determine the RANGAP1 levels through ELISA. In addition, various clinical, analytical, and echocardiographic variables, as well as endomyocardial biopsy results, were collected. RANGAP1 levels were higher in patients who developed ACR (median 63.15 ng/mL; (inter-quartile range (IQR), 36.61-105.69) vs. 35.33 ng/mL (IQR, 19.18-64.59); = 0.02). Receiver operating characteristic (ROC) curve analysis confirmed that RANGAP1 differentiated between patients with and without ACR (area under curve (AUC), 0.70; = 0.02), and a RANGAP1 level exceeding the cut-off point (≥90 ng/mL) was identified as a risk factor for the development of ACR (OR, 6.8; = 0.006). Two independent predictors of ACR identified in this study were higher RANGAP1 and N-terminal pro-brain natriuretic peptide levels. The analysis of the ROC curve of the model showed a significant AUC of 0.77, = 0.001. Our findings suggest that RANGAP1 quantification facilitates risk prediction for the occurrence of ACR and could be considered as a novel non-invasive biomarker of ACR.
急性细胞排斥反应(ACR)的非侵入性诊断是一项重大挑战。我们开展了一项分子研究,分析血清RanGTP酶AP1(RANGAP1)在心脏移植(HT)后第一年诊断ACR的预测能力。我们纳入了75例连续的HT患者的血清样本,这些样本在临床稳定后采集,通过酶联免疫吸附测定(ELISA)确定RANGAP1水平。此外,还收集了各种临床、分析和超声心动图变量以及心内膜心肌活检结果。发生ACR的患者RANGAP1水平较高(中位数为63.15 ng/mL;四分位间距(IQR)为36.61 - 105.69),而未发生ACR的患者为35.33 ng/mL(IQR为19.18 - 64.59);P = 0.02)。受试者工作特征(ROC)曲线分析证实,RANGAP1能够区分发生ACR和未发生ACR的患者(曲线下面积(AUC)为0.70;P = 0.02),并且RANGAP1水平超过临界点(≥90 ng/mL)被确定为发生ACR的危险因素(比值比(OR)为6.8;P = 0.006)。本研究中确定的ACR的两个独立预测因素是较高的RANGAP1和N末端脑钠肽前体水平。该模型的ROC曲线分析显示AUC显著为0.77,P = 0.001。我们的研究结果表明,RANGAP1定量有助于预测ACR发生的风险,可被视为ACR的一种新型非侵入性生物标志物。