HUH Heart and Lung Center, University of Helsinki and Helsinki University Hospital, (Haartmaninkatu 4), P.O. Box 372, 00029, Helsinki, Finland.
Doctoral Programme in Clinical Research, University of Helsinki, Helsinki, Finland.
BMC Pulm Med. 2022 Jun 25;22(1):248. doi: 10.1186/s12890-022-02044-5.
Chronic respiratory failure (CRF) can be treated at home with non-invasive ventilation (NIV) and/or long-term oxygen (LTOT). The prevalence of these treatments is largely unknown. We aimed to clarify the prevalence and indications of the treatments, and the three-year mortality of the treated patients in the Helsinki University Hospital (HUH) area in Finland.
In this retrospective study we analyzed the prevalence of adult CRF patients treated with NIV and/or LTOT on 1.1.2018 and followed these patients until 1.1.2021. Data collected included the underlying diagnosis, patient characteristics, information on treatment initiation and from the last follow-up visit, and mortality during the three-year follow-up. Patients with home invasive mechanical ventilation or sleep apnea were excluded.
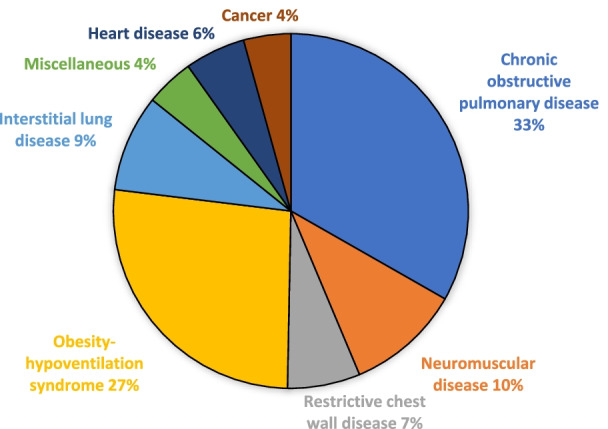
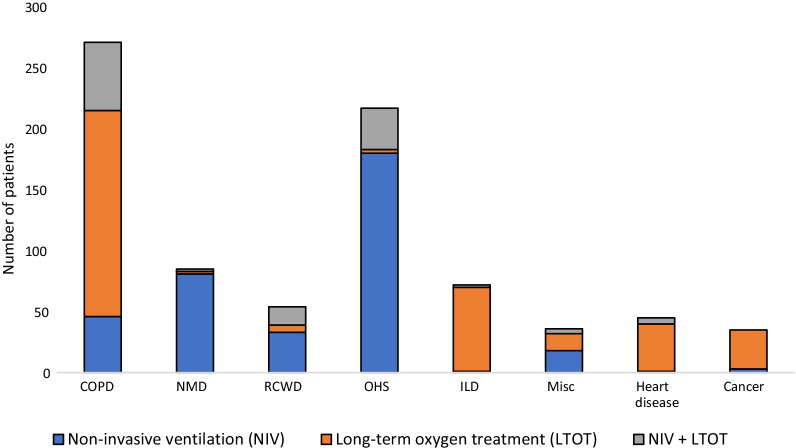
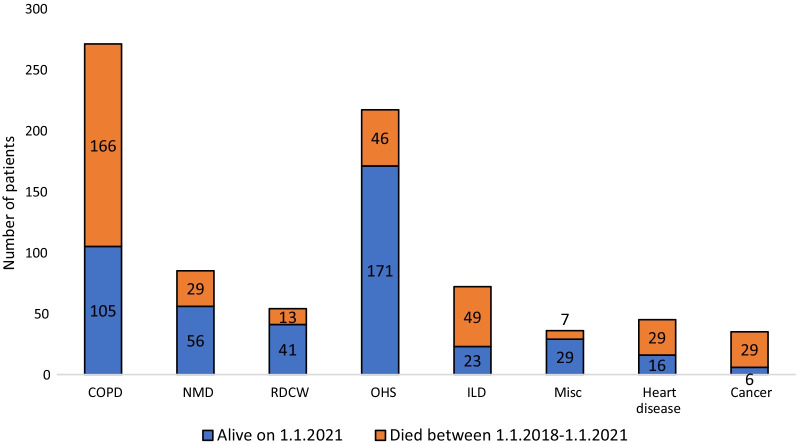
On 1.1.2018, we had a total of 815 patients treated with NIV and/or LTOT in the Helsinki University Hospital (HUH) area, with a population of 1.4 million. The prevalence of NIV was 35.4 per 100,000, of LTOT 24.6 per 100,000 and of the treatments combined 60.0 per 100,000. Almost half, 44.5%, were treated with NIV, 41.0% with LTOT, and 14.4% underwent both. The most common diagnostic groups were chronic obstructive pulmonary disease (COPD) (33.3%) and obesity-hypoventilation syndrome (OHS) (26.6%). The three-year mortality in all patients was 45.2%. In the COPD and OHS groups the mortality was 61.3% and 21.2%. In NIV treated patients, the treatment durations varied from COPD patients 5.3 years to restrictive chest wall disease patients 11.4 years. The age-adjusted Charlson co-morbidity index (ACCI) median for all patients was 3.0.
NIV and LTOT are common treatments in CRF. The prevalence in HUH area was comparable to other western countries. As the ACCI index shows, the treated patients were fragile, with multiple co-morbidities, and their mortality was high. Treatment duration and survival vary greatly depending on the underlying diagnosis.
慢性呼吸衰竭(CRF)可以通过无创通气(NIV)和/或长期氧疗(LTOT)进行家庭治疗。这些治疗的流行程度在很大程度上是未知的。我们旨在阐明芬兰赫尔辛基大学医院(HUH)地区治疗患者的治疗方法的流行程度和适应症,以及治疗患者的三年死亡率。
在这项回顾性研究中,我们分析了 2018 年 1 月 1 日接受 NIV 和/或 LTOT 治疗的成年 CRF 患者的流行率,并对这些患者进行了随访,直到 2021 年 1 月 1 日。收集的数据包括潜在诊断、患者特征、治疗开始和最近一次随访的信息,以及三年随访期间的死亡率。排除了在家中接受有创机械通气或睡眠呼吸暂停治疗的患者。
2018 年 1 月 1 日,我们在赫尔辛基大学医院(HUH)地区共有 815 名患者接受 NIV 和/或 LTOT 治疗,人口为 140 万。NIV 的流行率为每 10 万人中有 35.4 人,LTOT 的流行率为每 10 万人中有 24.6 人,联合治疗的流行率为每 10 万人中有 60.0 人。近一半(44.5%)接受 NIV 治疗,41.0%接受 LTOT 治疗,14.4%同时接受两种治疗。最常见的诊断组是慢性阻塞性肺疾病(COPD)(33.3%)和肥胖低通气综合征(OHS)(26.6%)。所有患者的三年死亡率为 45.2%。在 COPD 和 OHS 组中,死亡率分别为 61.3%和 21.2%。在接受 NIV 治疗的患者中,治疗持续时间从 COPD 患者的 5.3 年到限制性胸壁疾病患者的 11.4 年不等。所有患者的年龄调整 Charlson 合并症指数(ACCI)中位数为 3.0。
NIV 和 LTOT 是 CRF 的常见治疗方法。在 HUH 地区的流行程度与其他西方国家相当。如 ACCI 指数所示,治疗患者身体脆弱,合并多种疾病,死亡率高。治疗持续时间和生存情况因潜在诊断而异。