Mach Tiffany, Qi Amy, Bouganim Nathaniel, Trinh Emilie
McGill University, Montreal, QC, Canada.
Division of Oncology, Department of Medicine, McGill University Health Center, Montreal, QC, Canada.
Can J Kidney Health Dis. 2022 Jun 21;9:20543581221106246. doi: 10.1177/20543581221106246. eCollection 2022.
Targeted cancer therapies have revolutionized the field of oncology by selecting for specific molecular pathways, thus improving overall clinical prognosis. However, many of these targeted treatments have been reported to have adverse kidney effects, including acute kidney injury, interstitial nephritis, and glomerular disease. Furthermore, some of these targeted therapies have also been found to cause an asymptomatic rise in serum creatinine levels through inhibition of active tubular secretion.
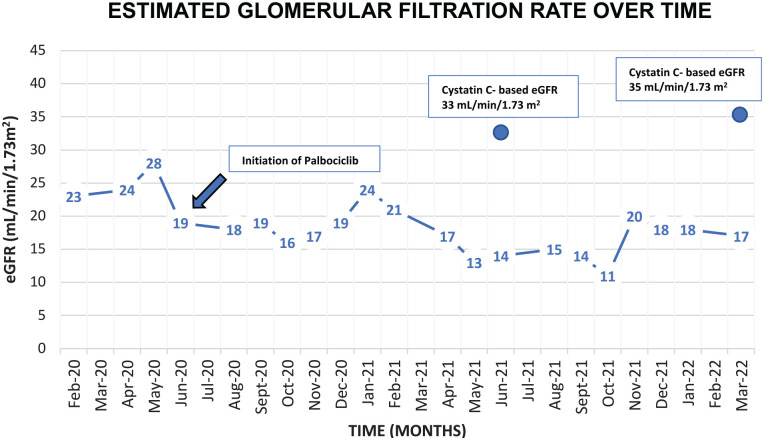
A 79-year-old woman was being followed for stage 4 A2 chronic kidney disease secondary to type 2 diabetes and longstanding hypertension. She was diagnosed with invasive mammary carcinoma and was initiated on letrozole, an aromatase inhibitor, and palbociclib, a selective cyclin-dependent kinase inhibitor, was subsequently added. Prior to the initiation of her treatments, her baseline estimated glomerular filtration rate (eGFR) fluctuated between 25 and 28 mL/min/1.73 m over the previous year. After initiating palbociclib, her serum creatinine progressively increased, despite having well-controlled blood pressure and diabetes. In addition, there was no history of pre-renal events nor any sonographic evidence of obstruction. Within 7 months, her eGFR based on serum creatinine had decreased down to 12 mL/min/1.73 m.
Given that there were no clinical or other biochemical changes suggestive of worsening renal function, a serum cystatin C was measured using an immunoturbidimetric assay, which was 1.71 mg/L and correlated with an eGFR of 33 mL/min/1.73 m based on the chronic kidney disease epidemiology collaboration (CKD-EPI) cystatin C equation (2012). This value was consistent with her previous baseline. Based on these findings, the significant decrease in eGFR measured by serum creatinine was attributed to the inhibitory effects of palbociclib on tubular creatinine secretion, rather than representing true kidney damage. Thus, a kidney biopsy was not performed in this context.
Seven months later, a repeat serum cystatin C was repeated to assess for any worsening of the patient's kidney function and revealed an eGFR of 35 mL/min/1.73 m based on the CKD-EPI cystatin C equation (2012), thus revealing stable kidney function and reinforcing the inhibitory effects of palbociclib on tubular creatinine secretion through its direct effects on kidney transporters.
This case report and literature review acknowledges the importance of using alternative methods of assessing kidney function when patients are undergoing targeted cancer therapies known to affect tubular creatinine secretion, which include cyclin-dependent kinase 4/6 inhibitors, poly(adenosine diphosphate-ribose) polymerase inhibitors, tyrosine kinase inhibitors, and mesenchymal-epithelial transition inhibitors. The use of non-creatinine-based markers of glomerular filtration rate (GFR), such as cystatin C and nuclear renal scans, will allow for more accurate estimation of kidney function in the appropriate setting, thus avoiding invasive diagnostic tests and unnecessary adjustments of treatment plans. However, certain targeted cancer therapies have also been proven to cause true kidney injury; therefore, physicians must still maintain a high degree of suspicion and consider invasive investigations and/or cessation or reduction of treatments when alternative measurements of kidney function do not suggest an underestimation of GFR via serum creatinine.

靶向癌症治疗通过选择特定的分子途径彻底改变了肿瘤学领域,从而改善了整体临床预后。然而,据报道,许多这些靶向治疗具有不良肾脏影响,包括急性肾损伤、间质性肾炎和肾小球疾病。此外,还发现其中一些靶向治疗通过抑制肾小管主动分泌导致血清肌酐水平无症状升高。
一名79岁女性因2型糖尿病和长期高血压继发4期A2慢性肾病而接受随访。她被诊断为浸润性乳腺癌,开始使用芳香化酶抑制剂来曲唑治疗,随后添加了选择性细胞周期蛋白依赖性激酶抑制剂哌柏西利。在开始治疗前,她的基线估计肾小球滤过率(eGFR)在过去一年中在25至28毫升/分钟/1.73平方米之间波动。开始使用哌柏西利后,尽管血压和糖尿病得到良好控制,但她的血清肌酐逐渐升高。此外,没有肾前事件史,也没有任何超声检查提示梗阻的证据。在7个月内,基于血清肌酐的eGFR降至12毫升/分钟/1.73平方米。
鉴于没有临床或其他生化变化提示肾功能恶化,使用免疫比浊法测量血清胱抑素C,结果为1.71毫克/升,根据慢性肾脏病流行病学合作组织(CKD - EPI)胱抑素C方程(2012年),其与eGFR为33毫升/分钟/1.73平方米相关。该值与她之前的基线一致。基于这些发现,血清肌酐测量的eGFR显著下降归因于哌柏西利对肾小管肌酐分泌的抑制作用,而不是代表真正的肾脏损伤。因此,在此情况下未进行肾活检。
7个月后,再次检测血清胱抑素C以评估患者肾功能是否恶化,根据CKD - EPI胱抑素C方程(2012年)显示eGFR为35毫升/分钟/1.73平方米,从而显示肾功能稳定,并强化了哌柏西利通过其对肾脏转运体的直接作用对肾小管肌酐分泌的抑制作用。
本病例报告和文献综述认识到,当患者接受已知会影响肾小管肌酐分泌的靶向癌症治疗时,使用替代方法评估肾功能的重要性,这些治疗包括细胞周期蛋白依赖性激酶4/6抑制剂、聚(二磷酸腺苷 - 核糖)聚合酶抑制剂、酪氨酸激酶抑制剂和间充质 - 上皮转化抑制剂。使用基于非肌酐的肾小球滤过率(GFR)标志物,如胱抑素C和核肾扫描,将在适当情况下更准确地估计肾功能,从而避免侵入性诊断测试和不必要的治疗计划调整。然而,某些靶向癌症治疗也已被证明会导致真正的肾损伤;因此,当肾功能的替代测量结果未提示通过血清肌酐低估GFR时,医生仍必须保持高度怀疑,并考虑进行侵入性检查和/或停止或减少治疗。