Thom Katharina, Kahl Beatrice, Wagner Thomas, van Egmond-Fröhlich Andreas, Krainz Mathias, Frischer Thomas, Leeb Iris, Schuster Christine, Ehringer-Schetitska Doris, Minkov Milen, Male Christoph, Michel-Behnke Ina
Department of Pediatrics, Division of Pediatric Cardiology, Pediatric Heart Centre, Medical University of Vienna, Vienna, Austria.
Department of Pediatrics and Adolescent Medicine, Clinic Donaustadt, Vienna, Austria.
Front Pediatr. 2022 Jun 10;10:896252. doi: 10.3389/fped.2022.896252. eCollection 2022.
comprises a new disease entity having emerged after the COVID-19 outbreak in 2019.
For this multicenter, retrospective study children between 0 and 18 years with PIMS-TS between March 2020 and May 2021 were included, before availability of vaccination for children. Frequent SARS-CoV-2 variants at that period were the wildtype virus, alpha, beta and delta variants. Inclusion criteria were according to the PIMS-TS criteria, proposed by the Royal College of Pediatrics and WHO. Study aim was to review their clinical, laboratory and echocardiographic data with a focus on cardiac involvement.
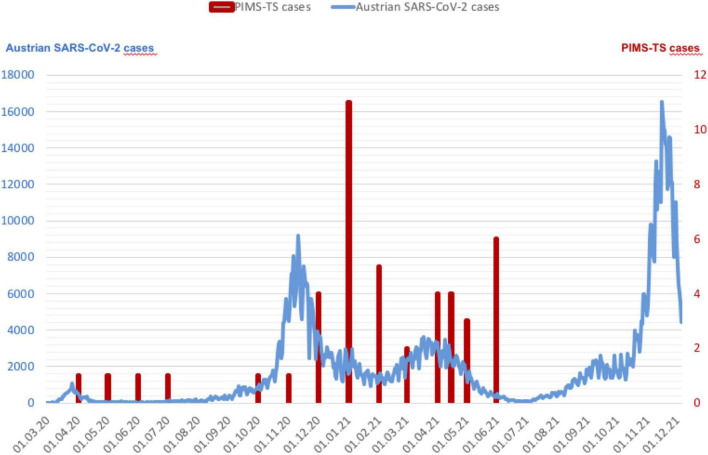
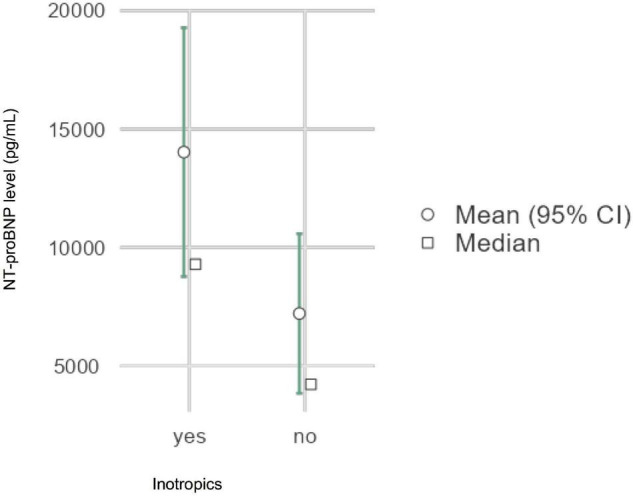
We report 45 patients, median age 9 years, 64% male. SARS-CoV-2 antibodies were positive in 35/41 (85%). PIMS occurrence followed local COVID-19 peak incidence periods with a time lag. The most common symptoms at presentation were fever (98%), abdominal pain (89%) and rash (80%). Fever history of > 5 days was associated with decreased left ventricular function ( = 0.056). Arterial hypotension and cardiac dysfunction were documented in 72% patients, increased brain natriuretic peptide in 96% and increased cardiac troponin in 64% of the children. Echocardiography revealed mitral valve regurgitation (64%), coronary abnormalities (36%) and pericardial effusions (40%). Increased NT-proBNP was significantly associated with the need of inotropics ( < 0.05), which were necessary in 40% of the patients. Treatment comprised intravenous immunoglobulin (93%), systemic steroids (84%) and acetylsalicylic acid (100%; 26/45 started with high dosages). For insufficient response to this treatment, five (11%) children received the interleukin-1 receptor antagonist anakinra. All patients were discharged with almost resolved cardiac signs.
Our analysis of non-vaccinated children with PIMS-TS demonstrates that a considerable number have associated myocarditis requiring intensive care and inotropic support. Most children showed adequate response to intravenous immunoglobulin and steroids and good recovery. Further evaluation of pediatric patients with COVID-19 associated diseases is required to evaluate the impact of new virus variants.
PIMS-TS是2019年新冠疫情爆发后出现的一种新的疾病实体。
在儿童可用疫苗之前,对2020年3月至2021年5月期间0至18岁患有PIMS-TS的儿童进行了这项多中心回顾性研究。当时常见的SARS-CoV-2变体为野生型病毒、α、β和δ变体。纳入标准依据皇家儿科学会和世界卫生组织提出的PIMS-TS标准。研究目的是回顾他们的临床、实验室和超声心动图数据,重点关注心脏受累情况。
我们报告了45例患者,中位年龄9岁,64%为男性。41例中有35例(85%)SARS-CoV-2抗体呈阳性。PIMS的发生在当地新冠疫情发病高峰期之后有一定时间滞后。就诊时最常见的症状为发热(98%)、腹痛(89%)和皮疹(80%)。发热超过5天与左心室功能下降相关(P = 0.056)。72%的患者记录有动脉低血压和心脏功能障碍,96%的儿童脑钠肽升高,64%的儿童心肌肌钙蛋白升高。超声心动图显示二尖瓣反流(64%)、冠状动脉异常(36%)和心包积液(40%)。NT-proBNP升高与需要使用正性肌力药物显著相关(P < 0.05),40%的患者需要使用。治疗包括静脉注射免疫球蛋白(93%)、全身用类固醇(84%)和阿司匹林(100%;45例中有26例起始为高剂量)。对于该治疗反应不佳的5例(11%)儿童接受了白细胞介素-1受体拮抗剂阿那白滞素。所有患者出院时心脏体征几乎均已消退。
我们对未接种疫苗的PIMS-TS儿童的分析表明,相当一部分患者伴有需要重症监护和正性肌力支持的心肌炎。大多数儿童对静脉注射免疫球蛋白和类固醇反应良好且恢复良好。需要对新冠相关疾病的儿科患者进行进一步评估,以评估新病毒变体的影响。