Akamatsu Hiroaki, Teraoka Shunsuke, Takamori Shinkichi, Miura Satoru, Hayashi Hidetoshi, Hata Akito, Toi Yukihiro, Shiraishi Yoshimasa, Mamesaya Nobuaki, Sato Yuki, Furuya Naoki, Oyanagi Jun, Koh Yasuhiro, Misumi Toshihiro, Yamamoto Nobuyuki, Nakagawa Kazuhiko
Internal Medicine III, Wakayama Medical University, Kimiidera, Wakayama, Japan.
Department of Thoracic Oncology, National Hospital Organization Kyushu Cancer Center, Notame, Minami-Ku, Fukuoka, Japan.
Clin Cancer Res. 2022 Jun 28;28(15):OF1-OF7. doi: 10.1158/1078-0432.CCR-22-0602.
To explore the efficacy of retreatment with immune checkpoint inhibitors (ICI) in patients with advanced non-small cell lung cancer (NSCLC) who responded to prior ICI and had adequate ICI-free interval.
Patients with advanced NSCLC who had achieved complete response (CR), partial response (PR), or stable disease for ≥6 months with prior ICI therapy preceding progression were prospectively enrolled. All patients should have had ICI-free interval ≥60 days before registration. Patients were treated with nivolumab (240 mg) every 2 weeks until progression. The primary endpoint was overall response rate (ORR). Secondary endpoints included progression-free survival (PFS), overall survival, and safety (Trial Identifier, UMIN000028561).
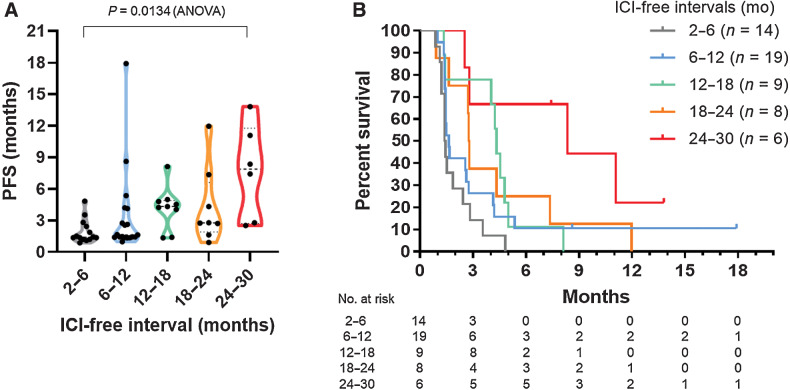
Sixty-one patients were enrolled during October 2017 to February 2020, with 59 analyzed for efficacy. Regarding prior ICI, 41 patients had CR or PR. Median treatment on ICI and median ICI-free intervals were 8.1 months and 9.2 months, respectively. Twenty patients experienced immune-related adverse events (irAE) that required discontinuation of prior ICI. Nivolumab retreatment demonstrated ORR of 8.5% [95% confidence interval (CI), 2.8-18.7%] and median PFS of 2.6 months (95% CI, 1.6-2.8 months) while 5 responders had 11.1 months of median PFS. In the multivariate analysis, ICI-free interval was the only predictive factor of PFS (HR, 2.02; P = 0.02), while prior efficacy or history of irAE was not. Common adverse events were skin disorders (23%), malaise (20%), and hypoalbuminemia (15%).
Even in patients who initially responded to prior ICI and had ICI-free interval, once resistance occurred, retreatment with nivolumab had limited efficacy.
探讨免疫检查点抑制剂(ICI)再治疗对既往接受ICI治疗有反应且有足够无ICI间期的晚期非小细胞肺癌(NSCLC)患者的疗效。
前瞻性纳入在疾病进展前接受过ICI治疗并达到完全缓解(CR)、部分缓解(PR)或疾病稳定≥6个月的晚期NSCLC患者。所有患者在登记前应有无ICI间期≥60天。患者每2周接受一次纳武利尤单抗(240mg)治疗,直至疾病进展。主要终点为总缓解率(ORR)。次要终点包括无进展生存期(PFS)、总生存期和安全性(试验标识符,UMIN000028561)。
2017年10月至2020年2月期间共纳入61例患者,其中59例进行了疗效分析。关于既往ICI治疗,41例患者达到CR或PR。ICI治疗的中位疗程和中位无ICI间期分别为8.1个月和9.2个月。20例患者发生了需要停用既往ICI的免疫相关不良事件(irAE)。纳武利尤单抗再治疗的ORR为8.5%[95%置信区间(CI),2.8 - 18.7%],中位PFS为2.6个月(95%CI,1.6 - 2.8个月),而5例缓解者的中位PFS为11.1个月。在多变量分析中,无ICI间期是PFS的唯一预测因素(风险比,2.02;P = 0.02),而既往疗效或irAE病史则不是。常见不良事件为皮肤疾病(23%)、不适(20%)和低白蛋白血症(15%)。
即使是最初对既往ICI治疗有反应且有无ICI间期的患者,一旦出现耐药,纳武利尤单抗再治疗的疗效也有限。