Tian Tian, Yu Min, Yu Yang, Wang Ke, Tian Panwen, Luo Ziyue, Ding Zhenyu, Wang Ye, Gong Youling, Zhu Jiang, Zou Bingwen, Sio Terence T, Alves Adelaide, Liu Yongmei, Huang Meijuan, Lu You
Department of Thoracic Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, China.
Department of Respiratory and Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, China.
Transl Lung Cancer Res. 2022 Jun;11(6):1027-1037. doi: 10.21037/tlcr-22-376.
Although immune checkpoint inhibitors (ICIs) provide unprecedented survival improvement for patients with advanced non-small cell lung cancer (NSCLC), disease progression inevitably occurs. After ICIs failure, limited data exist on whether ICI-based treatment beyond progression (TBP) may be beneficial to advanced NSCLC. This retrospective study aimed to evaluate the efficacy of this treatment approach in advanced NSCLC and identify potential beneficial factors.
Patients with stage IV NSCLC who received ICI-based treatment after the failure of prior PD-1/PD-L1 inhibitor treatments (monotherapy or combination therapy) between January 2016 and July 2020 were enrolled. Their clinical characteristics and treatment procedures were collected, and the follow-up would be performed.
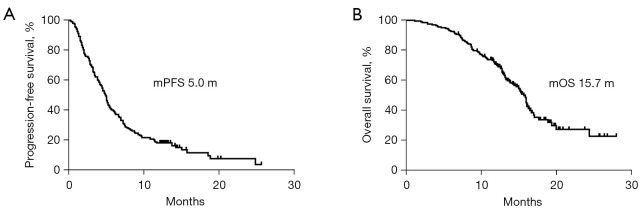
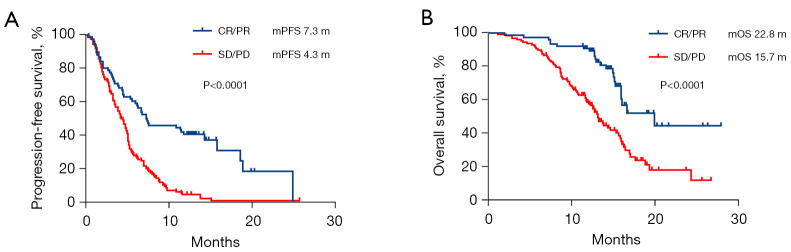
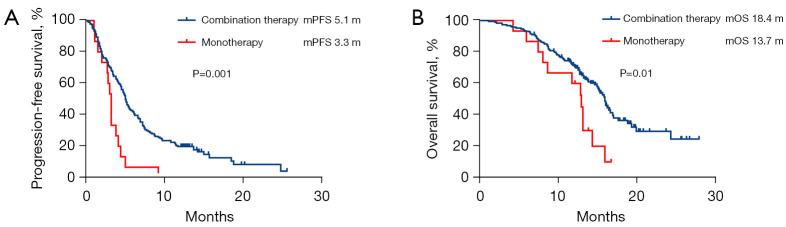
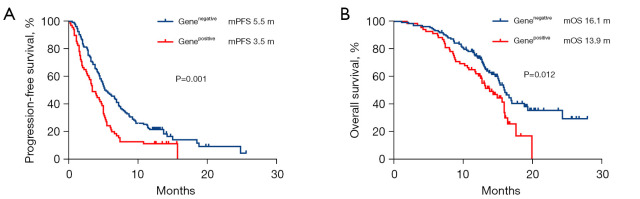
A total of 204 patients were included. All patients had disease progression after prior immunotherapy, with 49.5% (101/204) of patients presenting with new metastasis lesions and the rest 50.5% (103/204) of patients' progression on originate lesions. Within the entire cohort, the median progression-free survival (PFS) and median overall survival (OS) of ICI-based TBP with prior immunotherapy were 5.0 months (95% CI: 4.5-5.5 months) and 15.7 months (95% CI: 14.7-16.8 months), respectively. The objective response rate (ORR) and disease control rate (DCR) were 9.3% and 74.0%, respectively. According to the multivariate analysis, ICI-based combination therapy [PFS: hazard ratio (HR), 0.48, 95% confidence interval (CI): 0.28-0.84, P=0.011] (OS: HR, 0.44, 95% CI: 0.23-0.85, P=0.014), not having targetable gene alterations (PFS: HR, 0.56, 95% CI: 0.40-0.79, P=0.001) (OS: HR, 0.57, 95% CI: 0.37-0.87, P=0.009), and good response to prior immunotherapy (PFS: HR, 0.36, 95% CI: 0.24-0.53, P<0.0001) (OS: HR, 0.31, 95% CI: 0.19-0.52, P<0.0001) were independently associated with improved PFS and OS. Moreover, disease progression due to appearances of new metastasis (OS: HR, 0.56, 95% CI: 0.37-0.84, P=0.005) was only associated with better OS.
While the ORR in patients with advanced NSCLC receiving ICI-based TBP with prior immunotherapy was limited, the DCR was relatively high in our study which is encouraging. ICI-based treatment strategy may be a reasonable option for patients who progressed from prior immunotherapy. Further prospective studies on larger sample size are warranted.
尽管免疫检查点抑制剂(ICI)为晚期非小细胞肺癌(NSCLC)患者带来了前所未有的生存改善,但疾病进展仍不可避免。在ICI治疗失败后,关于进展后基于ICI的治疗(TBP)是否对晚期NSCLC有益的数据有限。这项回顾性研究旨在评估这种治疗方法在晚期NSCLC中的疗效,并确定潜在的有益因素。
纳入2016年1月至2020年7月期间在先期PD-1/PD-L1抑制剂治疗(单药治疗或联合治疗)失败后接受基于ICI治疗的IV期NSCLC患者。收集他们的临床特征和治疗过程,并进行随访。
共纳入204例患者。所有患者在先期免疫治疗后均出现疾病进展,其中49.5%(101/204)的患者出现新的转移病灶,其余50.5%(103/204)的患者在原发灶进展。在整个队列中,在先期免疫治疗基础上基于ICI的TBP的中位无进展生存期(PFS)和中位总生存期(OS)分别为5.0个月(95%CI:4.5-5.5个月)和15.7个月(95%CI:14.7-16.8个月)。客观缓解率(ORR)和疾病控制率(DCR)分别为9.3%和74.0%。根据多因素分析,基于ICI的联合治疗[PFS:风险比(HR),0.48,95%置信区间(CI):0.28-0.84,P=0.011](OS:HR,0.44,95%CI:0.23-0.85,P=0.014)、无可靶向基因改变(PFS:HR,0.56,95%CI:0.40-0.79,P=0.001)(OS:HR,0.57,95%CI:0.37-0.87,P=0.009)以及在先期免疫治疗中有良好反应(PFS:HR,0.36,95%CI:0.24-0.53,P<0.0001)(OS:HR,0.31,95%CI:0.19-0.52,P<0.0001)与PFS和OS改善独立相关。此外,因出现新转移而导致的疾病进展(OS:HR,0.56,95%CI:0.37-0.84,P=0.005)仅与较好的OS相关。
虽然在先期免疫治疗基础上接受基于ICI的TBP的晚期NSCLC患者的ORR有限,但在我们的研究中DCR相对较高,这令人鼓舞。基于ICI的治疗策略可能是在先期免疫治疗后进展的患者的合理选择。有必要对更大样本量进行进一步的前瞻性研究。