Mohn Medical Imaging and Visualization Centre (MMIV), Department of Radiology, Haukeland University Hospital, Bergen, Norway.
Section for Radiology, Department of Clinical Medicine, University of Bergen, Bergen, Norway.
Eur Radiol. 2023 Jan;33(1):221-232. doi: 10.1007/s00330-022-08949-3. Epub 2022 Jun 28.
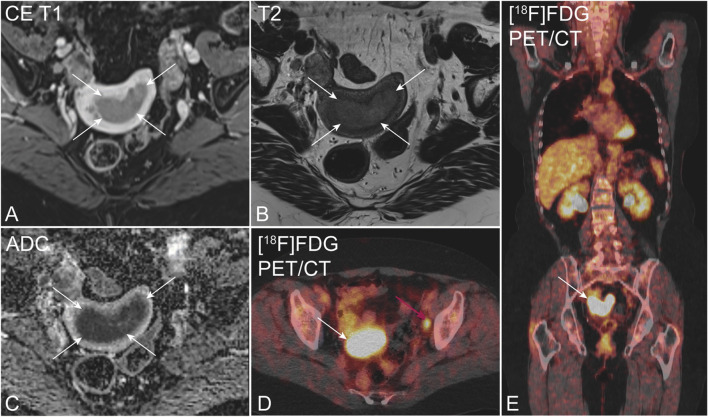
This study presents the diagnostic performance of four different preoperative imaging workups (IWs) for prediction of lymph node metastases (LNMs) in endometrial cancer (EC): pelvic MRI alone (IW1), MRI and [F]FDG-PET/CT in all patients (IW2), MRI with selective [F]FDG-PET/CT if high-risk preoperative histology (IW3), and MRI with selective [F]FDG-PET/CT if MRI indicates FIGO stage ≥ 1B (IW4).
In 361 EC patients, preoperative staging parameters from both pelvic MRI and [F]FDG-PET/CT were recorded. Area under receiver operating characteristic curves (ROC AUC) compared the diagnostic performance for the different imaging parameters and workups for predicting surgicopathological FIGO stage. Survival data were assessed using Kaplan-Meier estimator with log-rank test.
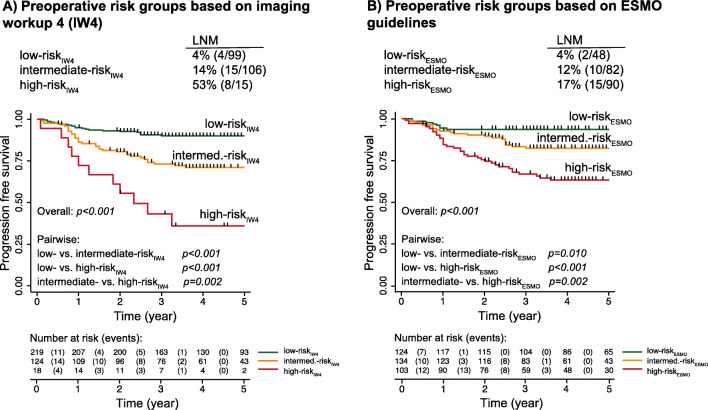
MRI and [F]FDG-PET/CT staging parameters yielded similar AUCs for predicting corresponding FIGO staging parameters in low-risk versus high-risk histology groups (p ≥ 0.16). The sensitivities, specificities, and AUCs for LNM prediction were as follows: IW1-33% [9/27], 95% [185/193], and 0.64; IW2-56% [15/27], 90% [174/193], and 0.73 (p = 0.04 vs. IW1); IW3-44% [12/27], 94% [181/193], and 0.69 (p = 0.13 vs. IW1); and IW4-52% [14/27], 91% [176/193], and 0.72 (p = 0.06 vs. IW1). IW3 and IW4 selected 34% [121/361] and 54% [194/361] to [F]FDG-PET/CT, respectively. Employing IW4 identified three distinct patient risk groups that exhibited increasing FIGO stage (p < 0.001) and stepwise reductions in survival (p ≤ 0.002).
Selective [F]FDG-PET/CT in patients with high-risk MRI findings yields better detection of LNM than MRI alone, and similar diagnostic performance to that of MRI and [F]FDG-PET/CT in all.
• Imaging by MRI and [F]FDG PET/CT yields similar diagnostic performance in low- and high-risk histology groups for predicting central FIGO staging parameters. • Utilizing a stepwise imaging workup with MRI in all patients and [F]FDG-PET/CT in selected patients based on MRI findings identifies preoperative risk groups exhibiting significantly different survival. • The proposed imaging workup selecting ~54% of the patients to [F]FDG-PET/CT yield better detection of LNMs than MRI alone, and similar LNM detection to that of MRI and [F]FDG-PET/CT in all.
本研究提出了四种不同术前影像学检查(IW)在预测子宫内膜癌(EC)淋巴结转移(LNM)中的诊断性能:盆腔 MRI 单独(IW1)、所有患者的 MRI 和 [F]FDG-PET/CT(IW2)、如果术前组织学为高危,则进行 MRI 和选择性 [F]FDG-PET/CT(IW3)、如果 MRI 提示 FIGO 分期≥1B,则进行 MRI 和选择性 [F]FDG-PET/CT(IW4)。
在 361 例 EC 患者中,记录了盆腔 MRI 和 [F]FDG-PET/CT 的术前分期参数。受试者工作特征曲线(ROC AUC)下的面积比较了不同成像参数和 IW 对预测手术病理 FIGO 分期的诊断性能。使用 Kaplan-Meier 估计器和对数秩检验评估生存数据。
MRI 和 [F]FDG-PET/CT 分期参数在低风险与高风险组织学组中预测相应的 FIGO 分期参数时具有相似的 AUC(p≥0.16)。LNM 预测的灵敏度、特异性和 AUC 如下:IW1-33%[9/27]、95%[185/193]和 0.64;IW2-56%[15/27]、90%[174/193]和 0.73(p=0.04 比 IW1);IW3-44%[12/27]、94%[181/193]和 0.69(p=0.13 比 IW1);IW4-52%[14/27]、91%[176/193]和 0.72(p=0.06 比 IW1)。IW3 和 IW4 分别将 34%[121/361]和 54%[194/361]的患者选择至 [F]FDG-PET/CT。采用 IW4 可识别出三个不同的患者风险组,这些组表现出 FIGO 分期的递增(p<0.001)和生存率的逐步降低(p≤0.002)。
在高危 MRI 发现的患者中进行选择性 [F]FDG-PET/CT 比单独 MRI 更能检测到 LNM,且与所有患者的 MRI 和 [F]FDG-PET/CT 具有相似的诊断性能。
MRI 和 [F]FDG-PET/CT 成像在预测中央 FIGO 分期参数方面,在低风险和高风险组织学组中具有相似的诊断性能。
采用逐步成像工作流程,所有患者均进行 MRI,根据 MRI 结果选择高危患者进行 [F]FDG-PET/CT,可识别出具有显著不同生存率的术前风险组。
选择约 54%的患者进行 [F]FDG-PET/CT 的建议成像工作流程,比单独 MRI 更能检测到 LNM,且与所有患者的 MRI 和 [F]FDG-PET/CT 具有相似的 LNM 检测性能。