Cantonal Hospital, Breast Center St Gallen, St Gallen, Switzerland.
University Hospital, Ulm, Germany.
J Clin Oncol. 2022 Sep 1;40(25):2946-2956. doi: 10.1200/JCO.21.02772. Epub 2022 Jun 28.
Combining standard of care (pertuzumab-trastuzumab [PH], chemotherapy) with cancer immunotherapy may potentiate antitumor immunity, cytotoxic activity, and patient outcomes in high-risk, human epidermal growth factor receptor 2 (HER2)-positive early breast cancer. We report the phase III IMpassion050 primary analysis of neoadjuvant atezolizumab, PH, and chemotherapy in these patients.
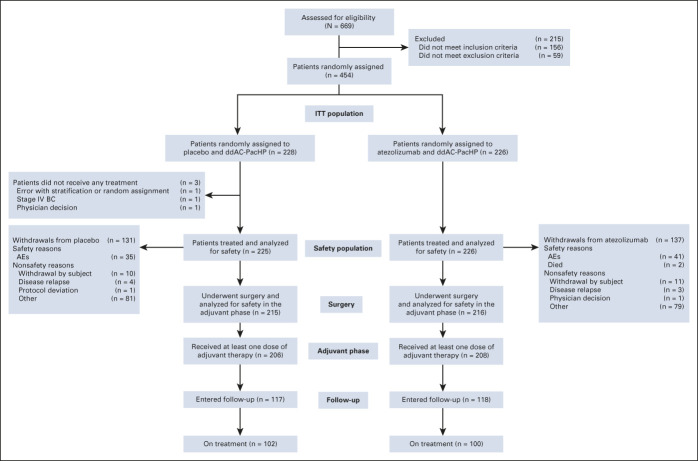
Patients with a primary tumor of > 2 cm and histologically confirmed, positive lymph node status (T2-4, N1-3, M0) were randomly assigned 1:1 to atezolizumab/placebo with dose-dense doxorubicin/cyclophosphamide, followed by paclitaxel, and PH. After surgery, patients were to continue atezolizumab/placebo and PH (total: 1 year of HER2-targeted therapy); those with residual disease could switch to ado-trastuzumab emtansine with atezolizumab/placebo. Coprimary efficacy end points were pathologic complete response (pCR; ypT0/is ypN0) rates in intention-to-treat (ITT) and programmed cell death-ligand 1 (PD-L1)-positive populations.
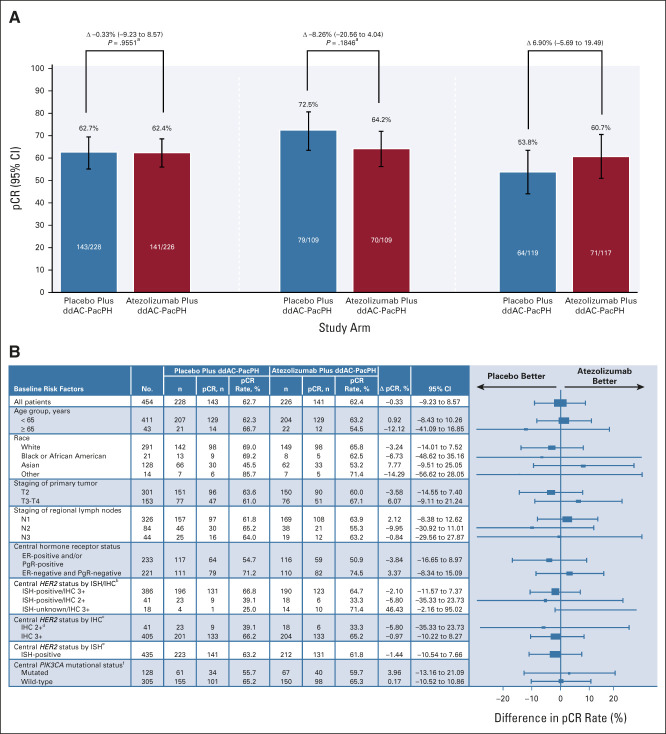
At clinical cutoff (February 5, 2021), pCR rates in the placebo and atezolizumab groups in the ITT populations were 62.7% (n = 143/228) and 62.4% (n = 141/226), respectively (difference -0.33%; 95% CI, -9.2 to 8.6; = .9551). The pCR rates in the placebo and atezolizumab groups in patients with PD-L1-positive tumors were 72.5% (n = 79/109) and 64.2% (n = 70/109), respectively (difference -8.26%; 95% CI, -20.6 to 4.0; = .1846). Grade 3-4 and serious adverse events were more frequent in the atezolizumab versus placebo group. Five grade 5 adverse events occurred (four neoadjuvant, one adjuvant; two assigned to study treatment), all with atezolizumab. Overall, the safety profile was consistent with that of atezolizumab in other combination studies.
Atezolizumab with neoadjuvant dose-dense doxorubicin/cyclophosphamide-paclitaxel and PH for high-risk, HER2-positive early breast cancer did not increase pCR rates versus placebo in the ITT or PD-L1-positive populations. PH and chemotherapy remains standard of care; longer follow-up may help to inform the long-term impact of atezolizumab.
在高风险、人表皮生长因子受体 2(HER2)阳性早期乳腺癌患者中,将标准治疗(曲妥珠单抗-帕妥珠单抗[PH]、化疗)与癌症免疫疗法相结合,可能增强抗肿瘤免疫、细胞毒性活性和患者结局。我们报告了 III 期 IMpassion050 研究中,新辅助阿替利珠单抗、PH 和化疗在这些患者中的初步分析结果。
患者的原发肿瘤>2cm,且组织学证实存在阳性淋巴结状态(T2-4、N1-3、M0),按 1:1 随机分配至阿替利珠单抗/安慰剂联合多西他赛、密集型多柔比星/环磷酰胺和紫杉醇,并给予 PH。手术后,患者继续接受阿替利珠单抗/安慰剂和 PH(共 1 年的 HER2 靶向治疗);有残留疾病的患者可以转为阿替利珠单抗联合 ado-trastuzumab emtansine。主要疗效终点为意向治疗(ITT)人群和程序性死亡配体 1(PD-L1)阳性人群的病理完全缓解(pCR;ypT0/is ypN0)率。
临床截止日期(2021 年 2 月 5 日)时,安慰剂组和阿替利珠单抗组在 ITT 人群中的 pCR 率分别为 62.7%(n=143/228)和 62.4%(n=141/226)(差异-0.33%;95%CI,-9.2 至 8.6;=0.9551)。PD-L1 阳性肿瘤患者中,安慰剂组和阿替利珠单抗组的 pCR 率分别为 72.5%(n=79/109)和 64.2%(n=70/109)(差异-8.26%;95%CI,-20.6 至 4.0;=0.1846)。阿替利珠单抗组的 3-4 级和严重不良事件更常见。5 例发生 5 级不良事件(4 例为新辅助治疗,1 例为辅助治疗;2 例分配至研究治疗),均与阿替利珠单抗相关。总体而言,安全性与阿替利珠单抗在其他联合研究中的安全性一致。
在高风险、HER2 阳性早期乳腺癌患者中,新辅助给予多西他赛、密集型多柔比星/环磷酰胺-紫杉醇和 PH 联合阿替利珠单抗,并未提高 ITT 或 PD-L1 阳性人群中的 pCR 率。PH 和化疗仍是标准治疗;更长时间的随访可能有助于了解阿替利珠单抗的长期影响。