Outcometrix, Salida, CO, USA.
Merck Healthcare KGaA, Darmstadt, Germany.
Patient. 2022 Nov;15(6):691-702. doi: 10.1007/s40271-022-00584-w. Epub 2022 Jun 30.
When determining if changes on patient-reported outcome (PRO) scores in clinical trials convey a meaningful treatment benefit, statistical significance tests alone may not communicate the patient perspective. Appraising within-patient changes on PRO scores against established thresholds can determine if improvements or deteriorations experienced by individuals are meaningful. To evaluate the appropriateness of thresholds for interpreting meaningful improvements and deterioration within individuals on the European Organisation for Research and Treatment of Cancer (EORTC) 30-item core instrument (QLQ-C30) and 13-item lung cancer module (QLQ-LC13), a series of psychometric methods were applied to data from a phase III randomized controlled clinical trial in non-small cell lung cancer.
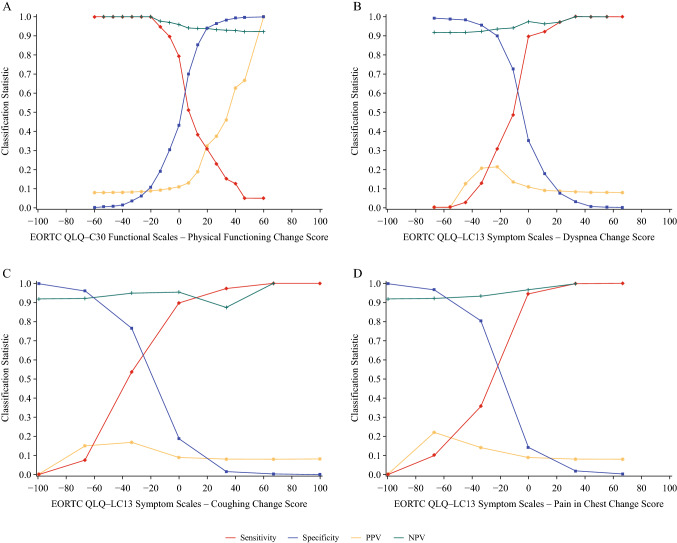
Anchor-based methods of empirical cumulative distribution functions and classification statistics were employed using change scores from Baseline to Week 7 using changes on the QLQ-C30 Global Health Status item as an anchor. Distribution-based methods of one-half standard deviation and standard error of measurement identified the minimum amount of change each domain score can reliably measure.
While the correlations between the domain scores and the anchor item were modest in size (i.e., r ≥ 0.30 for only 5 of 24 domains), consideration of multiple methods along with the magnitude of possible step changes on the score allowed for patterns to emerge. The triangulation process planned a priori resulted in different methods being the source for different domain scores. Absolute values of the proposed thresholds ranged from 11.11 to 33.33, and all resulted in the same classifications for all EORTC domains, except QLQ-C30 Fatigue, as would the 10-point threshold that is traditionally used.
This study confirms the appropriateness of the 10-point EORTC score threshold generally used by the field for interpreting within-patient changes, but the thresholds proposed from this study enhance interpretability by corresponding to only observable locations along the domain score scale.
在临床试验中,当确定患者报告结局(PRO)评分的变化是否具有有意义的治疗益处时,仅进行统计学显著性检验可能无法传达患者的观点。评估 PRO 评分的个体内变化是否超过既定阈值,可以确定个体经历的改善或恶化是否具有意义。为了评估欧洲癌症研究与治疗组织(EORTC)30 项核心量表(QLQ-C30)和 13 项肺癌模块(QLQ-LC13)用于解释个体内有意义的改善和恶化的阈值是否合适,采用了一系列心理测量方法,对非小细胞肺癌 III 期随机对照临床试验的数据进行了分析。
使用基于分布的方法,即基于基线至第 7 周的变化分数,使用 QLQ-C30 全球健康状况项目的变化作为锚点,采用经验累积分布函数和分类统计的基于锚点的方法。基于分布的方法使用一半标准差和测量误差标准确定每个域分数可以可靠测量的最小变化量。
虽然域分数与锚定项目之间的相关性较小(即,只有 24 个域中的 5 个域的 r 值≥0.30),但考虑多种方法以及分数上可能发生的阶跃变化的幅度,可以发现一些模式。预先计划的三角剖分过程导致不同的方法成为不同域分数的来源。所提出的阈值的绝对值范围为 11.11 到 33.33,除了 QLQ-C30 疲劳量表外,所有这些阈值都与传统使用的 10 分阈值一样,适用于所有 EORTC 域的分类。
这项研究证实了该领域通常用于解释个体内变化的 10 分 EORTC 评分阈值的适当性,但本研究提出的阈值通过与域评分尺度上仅可观察到的位置相对应,提高了可解释性。