Department of Gastroenterology and Hepatology, Leiden University Medical Center, Albinusdreef 2, 2333 ZA, Leiden, The Netherlands.
Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, The Netherlands.
Surg Endosc. 2022 Dec;36(12):9156-9168. doi: 10.1007/s00464-022-09396-3. Epub 2022 Jun 30.
T1 rectal cancer (RC) patients are increasingly being treated by local resection alone but uniform surveillance strategies thereafter are lacking. To determine whether different local resection techniques influence the risk of recurrence and cancer-related mortality, a meta-analysis was performed.
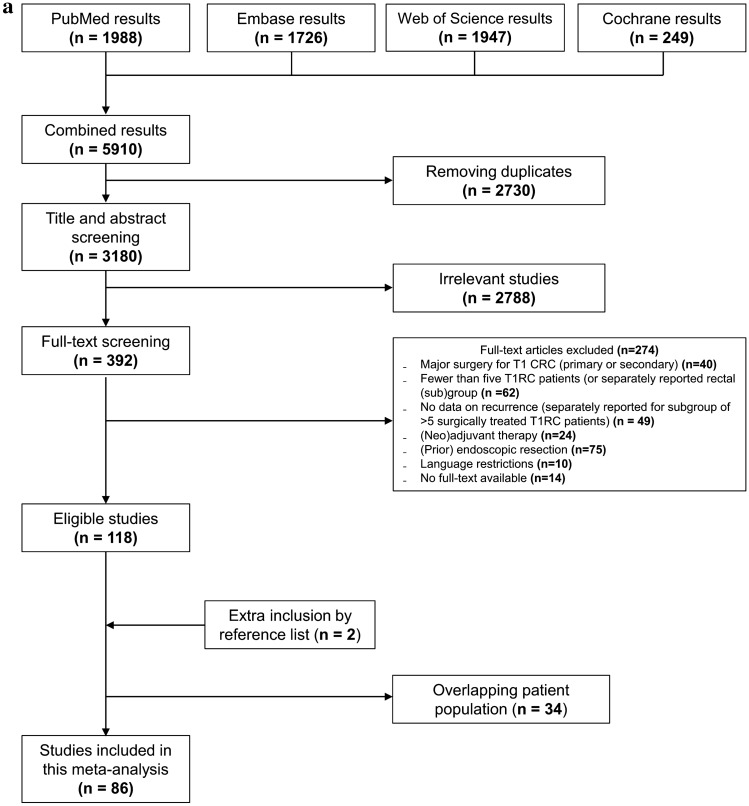
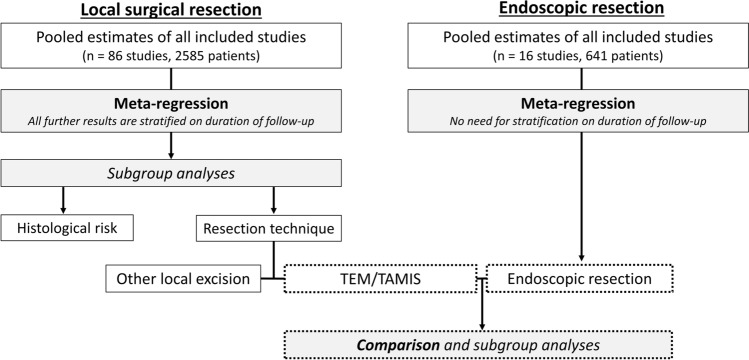
A systematic search was conducted for T1RC patients treated with local surgical resection. The primary outcome was the risk of RC recurrence and RC-related mortality. Pooled estimates were calculated using mixed-effect logistic regression. We also systematically searched and evaluated endoscopically treated T1RC patients in a similar manner.
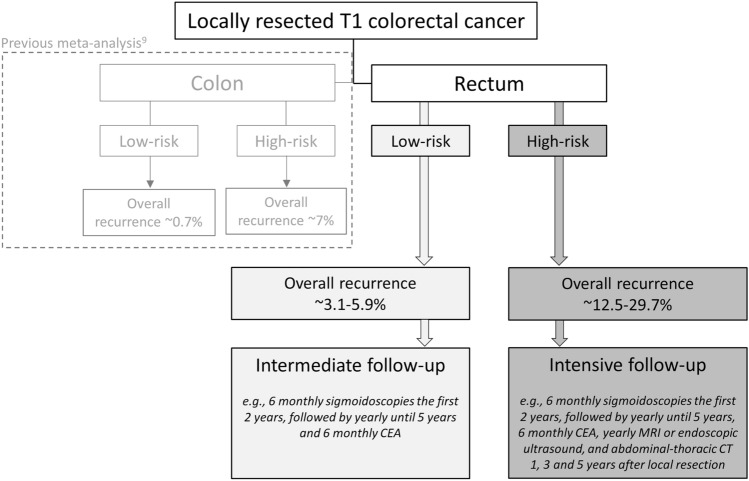
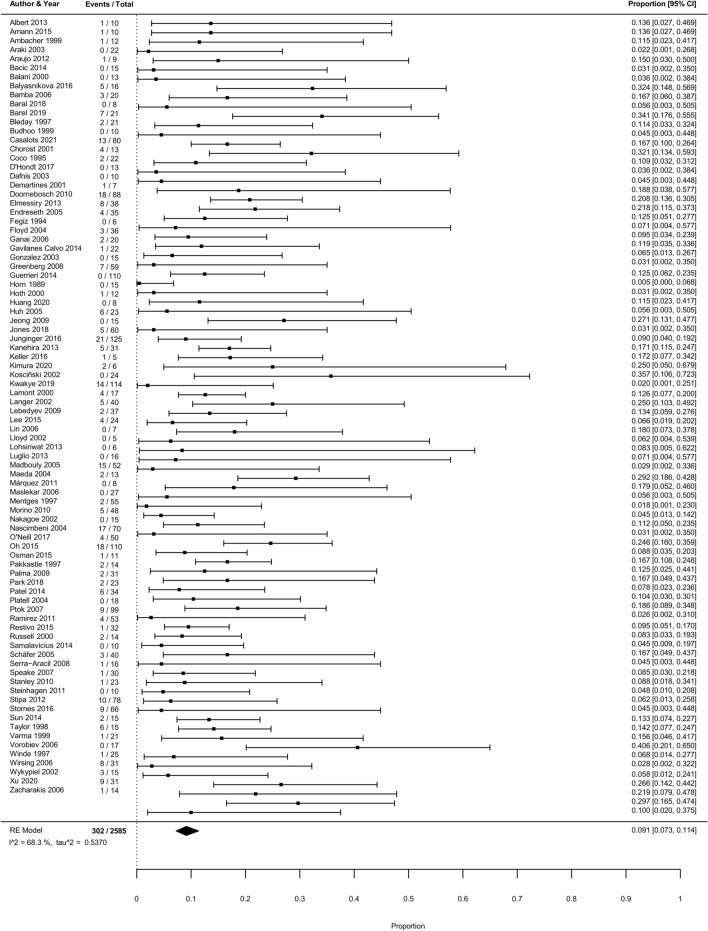
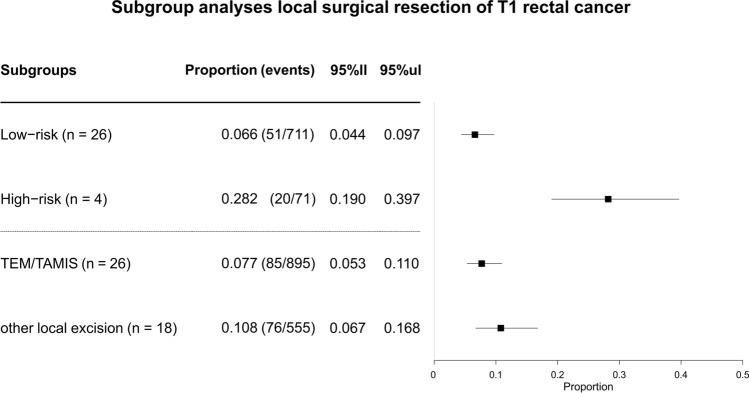
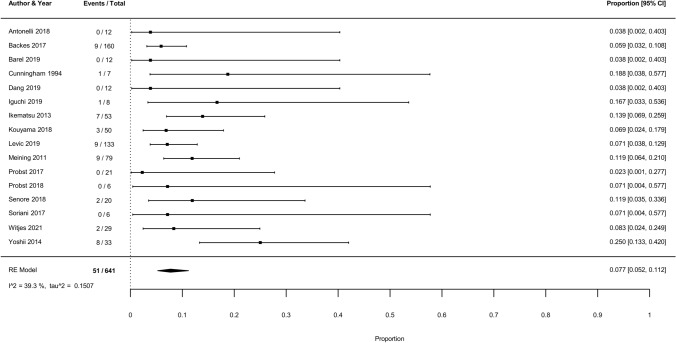
In 2585 unique T1RC patients (86 studies) undergoing local surgical resection, the overall pooled cumulative incidence of recurrence was 9.1% (302 events, 95% CI 7.3-11.4%; I = 68.3%). In meta-regression, the recurrence risk was associated with histological risk status (p < 0.005; low-risk 6.6%, 95% CI 4.4-9.7% vs. high-risk 28.2%, 95% CI 19-39.7%) and local surgical resection technique (p < 0.005; TEM/TAMIS 7.7%, 95% CI 5.3-11.0% vs. other local surgical excisions 10.8%, 95% CI 6.7-16.8%). In 641 unique T1RC patients treated with flexible endoscopic excision (16 studies), the risk of recurrence (7.7%, 95% CI 5.2-11.2%), cancer-related mortality (2.3%, 95% CI 1.1-4.9), and cancer-related mortality among patients with recurrence (30.0%, 95% CI 14.7-49.4%) were comparable to outcomes after TEM/TAMIS (risk of recurrence 7.7%, 95% CI 5.3-11.0%, cancer-related mortality 2.8%, 95% CI 1.2-6.2% and among patients with recurrence 35.6%, 95% CI 21.9-51.2%).
Patients with T1 rectal cancer may have a significantly lower recurrence risk after TEM/TAMIS compared to other local surgical resection techniques. After TEM/TAMIS and endoscopic resection the recurrence risk, cancer-related mortality and cancer-related mortality among patients with recurrence were comparable. Recurrence was mainly dependent on histological risk status.
越来越多的 T1 直肠肿瘤 (RC) 患者接受局部切除术治疗,但缺乏统一的监测策略。为了确定不同的局部切除技术是否会影响复发和与癌症相关的死亡率的风险,我们进行了一项荟萃分析。
系统地搜索了接受局部手术切除的 T1RC 患者。主要结局是 RC 复发和 RC 相关死亡率的风险。使用混合效应逻辑回归计算汇总估计值。我们还以类似的方式系统地搜索和评估了接受内镜治疗的 T1RC 患者。
在 2585 名接受局部手术切除的 T1RC 患者 (86 项研究) 中,总的累积复发率为 9.1%(302 例,95%CI 7.3-11.4%;I=68.3%)。在荟萃回归中,复发风险与组织学风险状况相关(p<0.005;低危组 6.6%,95%CI 4.4-9.7% vs. 高危组 28.2%,95%CI 19-39.7%)和局部手术切除技术(p<0.005;TEM/TAMIS 7.7%,95%CI 5.3-11.0% vs. 其他局部手术切除 10.8%,95%CI 6.7-16.8%)。在 641 名接受灵活内镜切除术治疗的 T1RC 患者 (16 项研究) 中,复发风险(7.7%,95%CI 5.2-11.2%)、癌症相关死亡率(2.3%,95%CI 1.1-4.9%)和复发患者的癌症相关死亡率(30.0%,95%CI 14.7-49.4%)与 TEM/TAMIS 后的结果相当(复发风险 7.7%,95%CI 5.3-11.0%,癌症相关死亡率 2.8%,95%CI 1.2-6.2%,复发患者的癌症相关死亡率 35.6%,95%CI 21.9-51.2%)。
与其他局部手术切除技术相比,TEM/TAMIS 后 T1 直肠肿瘤患者的复发风险显著降低。在 TEM/TAMIS 和内镜切除后,复发风险、癌症相关死亡率和复发患者的癌症相关死亡率相当。复发主要取决于组织学风险状况。