Albin Owen R, Saravolatz Louis, Petrie Joshua, Henig Oryan, Kaye Keith S
Department of Internal Medicine, University of Michigan Medical School, Ann Arbor, Michigan, USA.
Department of Epidemiology, University of Michigan School of Public Health, Ann Arbor, Michigan, USA.
Open Forum Infect Dis. 2022 Apr 14;9(6):ofac183. doi: 10.1093/ofid/ofac183. eCollection 2022 Jun.
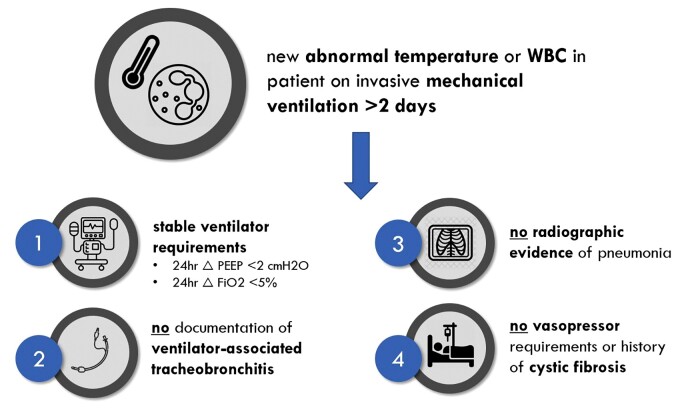
Respiratory cultures are often obtained as part of a "pan-culture" in mechanically ventilated patients in response to new fevers or leukocytosis, despite an absence of clinical or radiographic evidence suggestive of pneumonia.
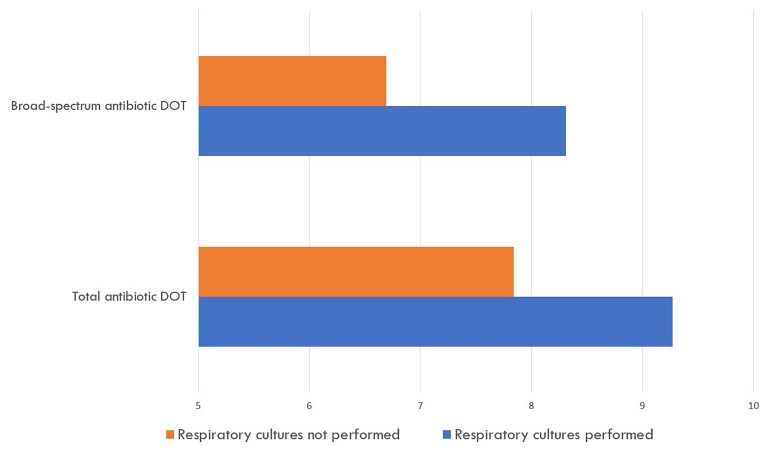
This was a propensity score-stratified cohort study of hospitalized mechanically ventilated adult patients between 2014 and 2019, with a new abnormal temperature or serum white blood cell count (NATW), but without radiographic evidence of pneumonia, change in ventilator requirements, or documentation of purulent secretions. Two patient groups were compared: those with respiratory cultures performed within 36 hours after NATW and those without respiratory cultures performed. The co-primary outcomes were the proportion of patients receiving >2 days of total antibiotic therapy and >2 days of broad-spectrum antibiotic therapy within 1 week after NATW.
Of 534 included patients, 113 (21.2%) had respiratory cultures obtained and 421 (78.8%) did not. Patients with respiratory cultures performed were significantly more likely to receive antibiotics for >2 days within 1 week after NATW than those without respiratory cultures performed (total antibiotic: adjusted odds ratio [OR], 2.57; 95% CI, 1.39-4.75; broad-spectrum antibiotic: adjusted OR, 2.47, 95% CI, 1.46-4.20).
Performance of respiratory cultures for fever/leukocytosis in mechanically ventilated patients without increasing ventilator requirements, secretion burden, or radiographic evidence of pneumonia was associated with increased antibiotic use within 1 week after incident abnormal temperature and/or white blood cell count. Diagnostic stewardship interventions targeting performance of unnecessary respiratory cultures in mechanically ventilated patients may reduce antibiotic overuse within intensive care units.
在机械通气患者中,尽管缺乏临床或影像学证据提示肺炎,但为应对新出现的发热或白细胞增多,常进行“全面培养”,其中包括呼吸道培养。
这是一项倾向评分分层队列研究,研究对象为2014年至2019年住院的机械通气成年患者,这些患者出现新的体温异常或血清白细胞计数异常(NATW),但无肺炎的影像学证据、呼吸机需求变化或脓性分泌物记录。比较了两组患者:一组是在NATW后36小时内进行呼吸道培养的患者,另一组是未进行呼吸道培养的患者。共同主要结局是在NATW后1周内接受>2天总抗生素治疗和>2天广谱抗生素治疗的患者比例。
在纳入的534例患者中,113例(21.2%)进行了呼吸道培养,421例(78.8%)未进行。与未进行呼吸道培养的患者相比,进行呼吸道培养的患者在NATW后1周内接受抗生素治疗>2天的可能性显著更高(总抗生素:调整后的优势比[OR],2.57;95%CI,1.39 - 4.75;广谱抗生素:调整后的OR,2.47,95%CI,1.46 - 4.20)。
在机械通气患者中,对于发热/白细胞增多且无呼吸机需求增加、分泌物负担增加或肺炎影像学证据的情况进行呼吸道培养,与在出现异常体温和/或白细胞计数后的1周内抗生素使用增加有关。针对机械通气患者不必要的呼吸道培养进行诊断管理干预,可能会减少重症监护病房内的抗生素过度使用。