Marzouki Sami, Peeters Bernard, Gevaert Sofie, Van Herzeele Isabelle
Department of Cardiovascular Radiology, Ghent University Hospital, Corneel Heymanslaan 10, 9000 Ghent, Belgium.
Department of Thoracic & Vascular Surgery, Ghent University Hospital, Corneel Heymanslaan 10, 9000 Ghent, Belgium.
Eur Heart J Case Rep. 2022 Jun 16;6(6):ytac238. doi: 10.1093/ehjcr/ytac238. eCollection 2022 Jun.
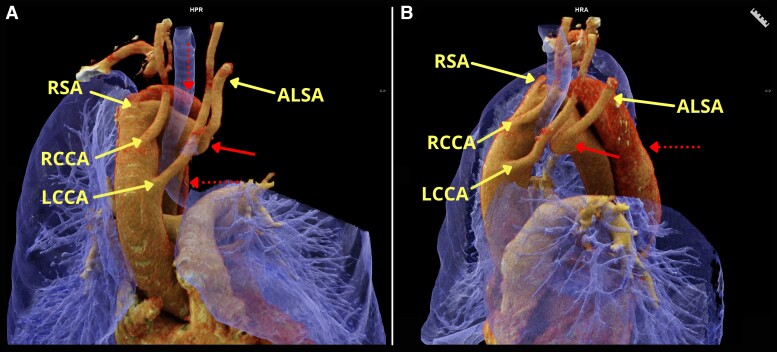
A right-sided aortic arch (RAArch) is present in approximately 0.1% of the population. A Kommerell's diverticulum (KD), a remnant of the dorsal aortic arch usually refers to an aneurysmal aortic enlargement at the origin of an aberrant left subclavian artery (ALSA) and is associated with an increased risk of aortic dissection.
A 59-year-old female smoker with a history of hypertension and hypercholesterolaemia presented with a 24-hour history of sudden-onset and severe stabbing chest pain radiating to the interscapular region. Physical examination was normal except for bilateral basal crepitations. Computed tomography angiography (CTA) showed a type B aortic dissection in a RAArch with an ALSA arising from KD with a peri-aortic haematoma and haemothorax without any active contrast extravasation. After medical stabilization, a semi-urgent hybrid repair was performed with a right carotid-subclavian bypass, thoracic endovascular aortic repair (TEVAR), a plug in the left subclavian artery, and left carotid-subclavian bypass due to severe ischaemia of the left arm. The postoperative CTA showed patent bypasses, aortic remodelling, and a minimal type IIa endoleak at the level of the ALSA.
In patients with a type B dissection and KD, hybrid repair including TEVAR is feasible after careful pre-operative assessment of the patient's unique anatomy and may reduce post-surgical morbidity and mortality compared to open surgery. Prophylactic repair may be considered in patients with an asymptomatic RAArch and KD.
约0.1%的人群存在右位主动脉弓(RAArch)。Kommerell憩室(KD)是背主动脉弓的残余部分,通常指异常左锁骨下动脉(ALSA)起始处的主动脉瘤样扩张,与主动脉夹层风险增加相关。
一名59岁有高血压和高胆固醇血症病史的吸烟女性,出现突发剧烈刺痛性胸痛24小时,疼痛放射至肩胛间区。体格检查除双侧肺底湿啰音外均正常。计算机断层扫描血管造影(CTA)显示RAArch合并B型主动脉夹层,ALSA起自KD,伴有主动脉周围血肿和血胸,无活动性造影剂外渗。经药物稳定病情后,因左臂严重缺血,行半急诊杂交修复术,包括右颈动脉 - 锁骨下动脉旁路移植术、胸主动脉腔内修复术(TEVAR)、左锁骨下动脉封堵及左颈动脉 - 锁骨下动脉旁路移植术。术后CTA显示旁路血管通畅、主动脉重塑,ALSA水平有极小的IIa型内漏。
对于B型夹层合并KD的患者,在仔细术前评估患者独特解剖结构后,包括TEVAR的杂交修复术是可行的,与开放手术相比,可能降低术后发病率和死亡率。对于无症状RAArch和KD的患者可考虑预防性修复。