BARDS-Health Economics and Decision Science, Merck & Co, Inc., Kenilworth, NJ, USA.
BARDS-Health Economics and Decision Science, Merck & Co, Inc., 770 Sumneytown Pike, West Point, PA, 19486, USA.
Pharmacoeconomics. 2022 Jul;40(7):699-714. doi: 10.1007/s40273-022-01168-0. Epub 2022 Jul 2.
Coronavirus disease 2019 (COVID-19) imposes a substantial and ongoing burden on the US healthcare system and society. Molnupiravir is a new oral antiviral for treating COVID-19 in outpatient settings. This study evaluated the cost-effectiveness profile of molnupiravir versus best supportive care in the treatment of adult patients with mild-to-moderate COVID-19 at risk of progression to severe disease, from a US payer's perspective.
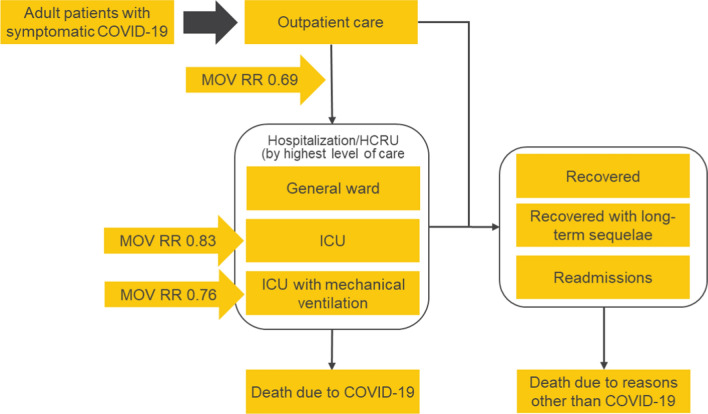
The model was developed using a decision tree for the short-term acute phase of COVID-19 and a Markov state transition model for the long-term post-acute phase. This model compared molnupiravir with best supportive care as consistent with the MOVe-OUT trial. Costs were reported in 2021 US dollars. Transition probabilities were derived from the phase III MOVe-OUT trial and the TriNetX real-world electronic health records database. Costs were derived from the TriNetX database and utility values from a de novo, vignette-based utility study. Deterministic and probabilistic sensitivity analyses (DSA/PSA) were conducted. Primary outcomes included proportion hospitalized, proportion who died overall and by highest healthcare setting at the end of the acute phase, quality-adjusted life-years (QALYs), and incremental costs per QALY gained over a lifetime (100 years) horizon, discounted at 3% annually and assessed at a willingness-to-pay (WTP) threshold of $100,000 per QALY.
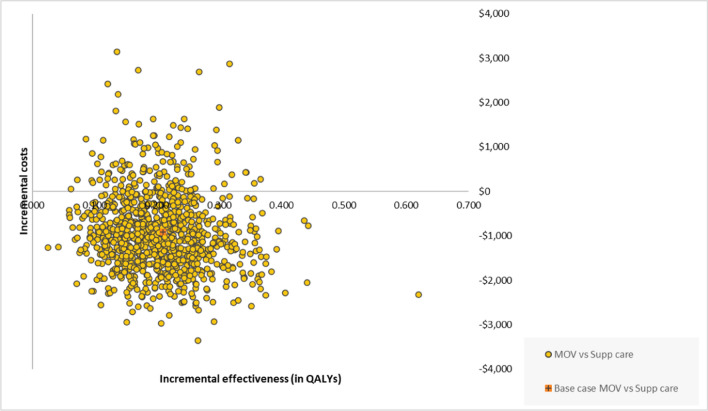
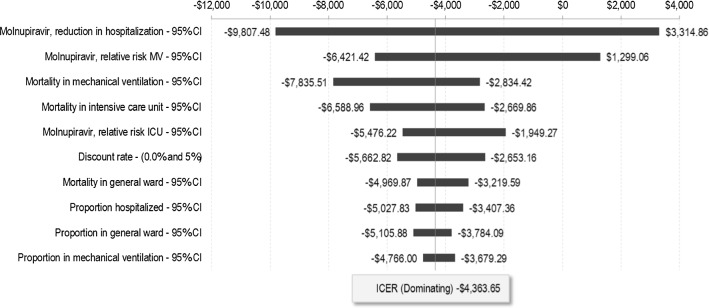
In this model, the use of molnupiravir led to an increase in QALYs (0.210) and decrease in direct total medical costs (-$895) per patient across a lifetime horizon, compared with best supportive care in COVID-19 outpatients. Molnupiravir was the dominant intervention when compared with best supportive care. Patients treated with molnupiravir were less likely to be hospitalized (6.38% vs. 9.20%) and more likely to remain alive (99.88% vs. 98.71%) during the acute phase. Through DSA, molnupiravir treatment effect of hospitalization reduction was identified to be the most influential parameter, and through PSA, molnupiravir remained dominant in 84% of the total simulations and, overall, 100% cost effective.
This analysis suggests that molnupiravir is cost effective compared with best supportive care for the treatment of adult outpatients with COVID-19. However, our study was limited by the unavailability of the most recent information on the rapidly evolving pandemic, including new viral variants, patient populations affected, and changes in standards of care. Further research should explore the impact of vaccination on the cost effectiveness of molnupiravir and other therapies, based on real-world data, to account for these changes, including the impact of vaccination and immunity.
2019 年冠状病毒病(COVID-19)给美国医疗保健系统和社会带来了巨大且持续的负担。莫努匹韦是一种新的口服抗病毒药物,用于治疗门诊环境中的 COVID-19。本研究从美国支付者的角度评估了莫努匹韦与最佳支持治疗在治疗有进展为重症风险的轻至中度 COVID-19 成年患者中的成本效益情况。
该模型使用决策树对 COVID-19 的短期急性期进行建模,使用马尔可夫状态转移模型对长期急性后期进行建模。该模型将莫努匹韦与最佳支持治疗进行了比较,这与 MOVe-OUT 试验一致。成本以 2021 年的美元报告。转移概率来自 III 期 MOVe-OUT 试验和 TriNetX 真实世界电子健康记录数据库。成本来自 TriNetX 数据库,效用值来自一项新的、基于情景的效用研究。进行了确定性和概率敏感性分析(DSA/PSA)。主要结果包括急性期中住院的比例、总体死亡比例以及最高医疗保健机构的死亡比例、质量调整生命年(QALYs)以及终生(100 年)获得的每个 QALY 的增量成本,按 3%的贴现率贴现,并在愿意支付(WTP)阈值为 100,000 美元/QALY 时进行评估。
在该模型中,与 COVID-19 门诊最佳支持治疗相比,莫努匹韦的使用导致每个患者的 QALYs 增加(0.210)和直接总医疗成本降低(-895 美元)。与最佳支持治疗相比,莫努匹韦是更具优势的干预措施。接受莫努匹韦治疗的患者在急性期中住院的可能性更低(6.38% vs. 9.20%),并且存活的可能性更高(99.88% vs. 98.71%)。通过 DSA,发现莫努匹韦对减少住院的治疗效果是最具影响力的参数,通过 PSA,莫努匹韦在 84%的总模拟中保持优势,并且总体上 100%具有成本效益。
与最佳支持治疗相比,本分析表明莫努匹韦在治疗 COVID-19 成年门诊患者方面具有成本效益。然而,我们的研究受到了迅速演变的大流行中最新信息的限制,包括新的病毒变体、受影响的患者人群以及护理标准的变化。进一步的研究应根据真实世界数据探索疫苗接种对莫努匹韦和其他疗法的成本效益的影响,以考虑这些变化,包括疫苗接种和免疫的影响。