Department of Social Policy and Intervention, University of Oxford, Oxford, UK.
Department of Social Policy and Intervention, University of Oxford, Oxford, UK.
Lancet Public Health. 2022 Jul;7(7):e638-e646. doi: 10.1016/S2468-2667(22)00133-5.
The effects of outsourcing health services to for-profit providers are contested, with some arguing that introducing such providers will improve performance through additional competition while others worry that this will lead to cost cutting and poorer outcomes for patients. We aimed to examine this debate by empirically evaluating the impact of outsourced spending to private providers, following the 2012 Health and Social Care Act, on treatable mortality rates and the quality of health-care services in England.
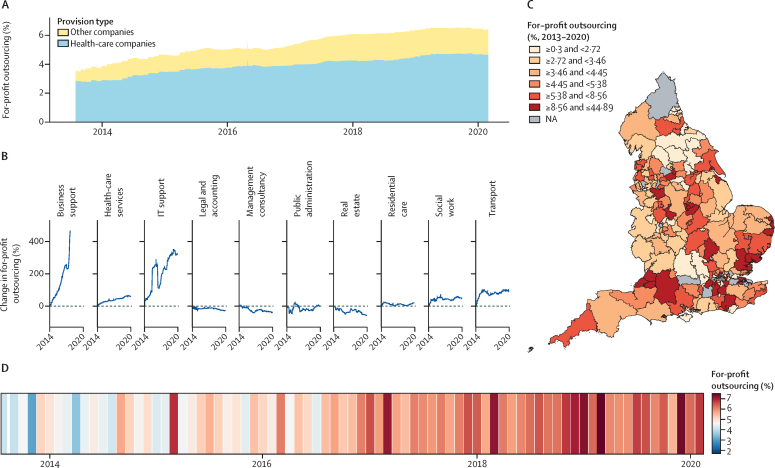
For this observational study, we used a novel database composed of parsable procurement contracts between April 1, 2013, and Feb 29, 2020 (n=645 674, value >£25 000, total value £204·1 billion), across 173 clinical commissioning groups (CCGs; regional health boards) in England. Data were compiled from 12 709 heterogenous expenditure files primarily scraped from commissioner websites with supplier names matched to registers identifying them as National Health Service (NHS) organisations, for-profit companies, or charities. We supplemented these data with rates of local mortality from causes that should be treatable by medical intervention, indicating the quality of health-care services. We used multivariate longitudinal regression models with fixed effects at the CCG level to analyse the association of for-profit outsourcing on treatable mortality rates in the following year. We used the average marginal effects to estimate total additional deaths attributable to changes in for-profit outsourcing. We provided alternative model specifications to test the robustness of our findings, match on background characteristics, examine the potential impact of measurement error, and adjust for possible confounding factors such as population demographics, total CCG expenditure, and local authority expenditure.
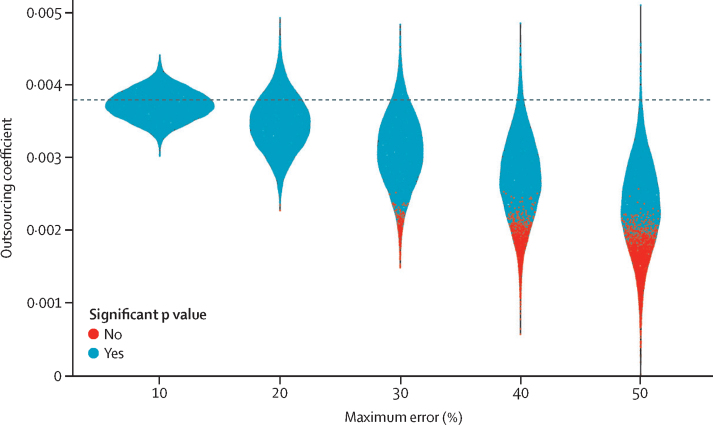
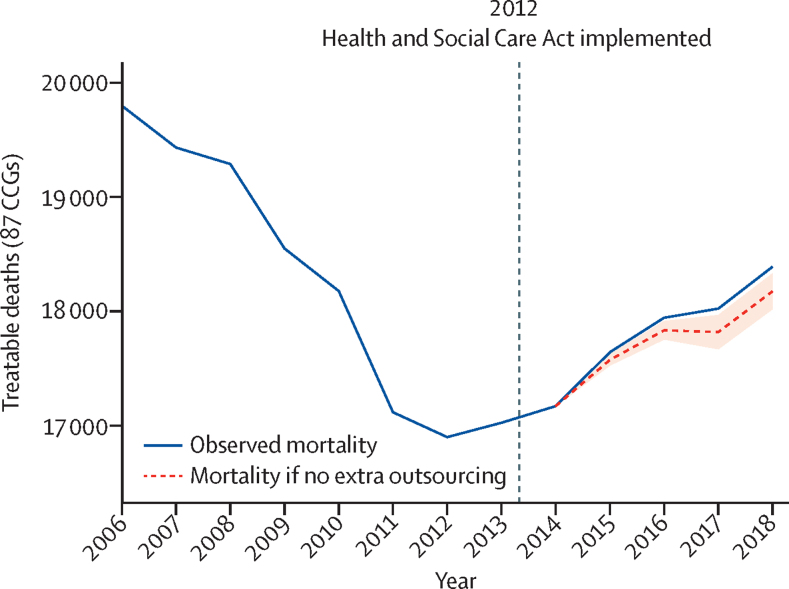
We found that an annual increase of one percentage point of outsourcing to the private for-profit sector corresponded with an annual increase in treatable mortality of 0·38% (95% CI 0·22-0·55; p=0·0016) or 0·29 (95% CI 0·09-0·49; p=0·0041) deaths per 100 000 population in the following year. This finding was robust to matching on background characteristics, adjusting for possible confounding factors, and measurement error in our dataset. Changes to for-profit outsourcing since 2014 were associated with an additional 557 (95% CI 153-961) treatable deaths across the 173 CCGs.
The privatisation of the NHS in England, through the outsourcing of services to for-profit companies, consistently increased in 2013-20. Private sector outsourcing corresponded with significantly increased rates of treatable mortality, potentially as a result of a decline in the quality of health-care services.
Wellcome Trust.
将医疗服务外包给营利性供应商的影响存在争议,一些人认为引入此类供应商将通过额外的竞争提高绩效,而另一些人则担心这将导致成本削减和患者预后恶化。我们旨在通过实证评估 2012 年《卫生和社会保健法案》之后外包给私人供应商的支出对英国可治疗死亡率和医疗服务质量的影响来检验这一争论。
在这项观察性研究中,我们使用了一个新颖的数据库,该数据库由 2013 年 4 月 1 日至 2020 年 2 月 29 日期间(n=645674,价值超过 25000 英镑,总价值 2041 亿英镑)的可解析采购合同组成,涵盖了英格兰 173 个临床委托组(CCG;区域卫生局)。数据主要从委员会网站上拼凑而成的 12709 个异构支出文件中收集,供应商名称与识别为国家卫生服务(NHS)组织、营利性公司或慈善机构的登记册相匹配。我们还利用当地可治疗死因的死亡率补充了这些数据,以表明医疗服务的质量。我们使用了在 CCG 层面具有固定效应的多变量纵向回归模型来分析次年营利性外包对可治疗死亡率的关联。我们使用平均边际效应来估计因营利性外包变化而导致的额外死亡总数。我们提供了替代模型规格来测试我们发现的稳健性,根据背景特征进行匹配,检查测量误差的潜在影响,并调整可能的混杂因素,如人口统计数据、CCG 总支出和地方当局支出。
我们发现,私营部门的外包比例每年增加一个百分点,与下一年可治疗死亡率每年增加 0.38%(95%CI 0.22-0.55;p=0.0016)或每 10 万人增加 0.29 人(95%CI 0.09-0.49;p=0.0041)相关。这一发现与根据背景特征进行匹配、调整可能的混杂因素以及我们数据集的测量误差有关。自 2014 年以来,营利性外包的变化与 173 个 CCG 中额外的 557 例(95%CI 153-961)可治疗死亡有关。
英格兰国民保健制度的私有化,通过将服务外包给营利性公司,在 2013-20 年期间持续增加。私营部门外包与可治疗死亡率的显著增加相关,这可能是医疗服务质量下降的结果。
惠康信托基金会。