Department of Ultrasound, The First Affiliated Hospital of Hainan Medical University, Haikou, China.
Front Endocrinol (Lausanne). 2022 Jun 17;13:899575. doi: 10.3389/fendo.2022.899575. eCollection 2022.
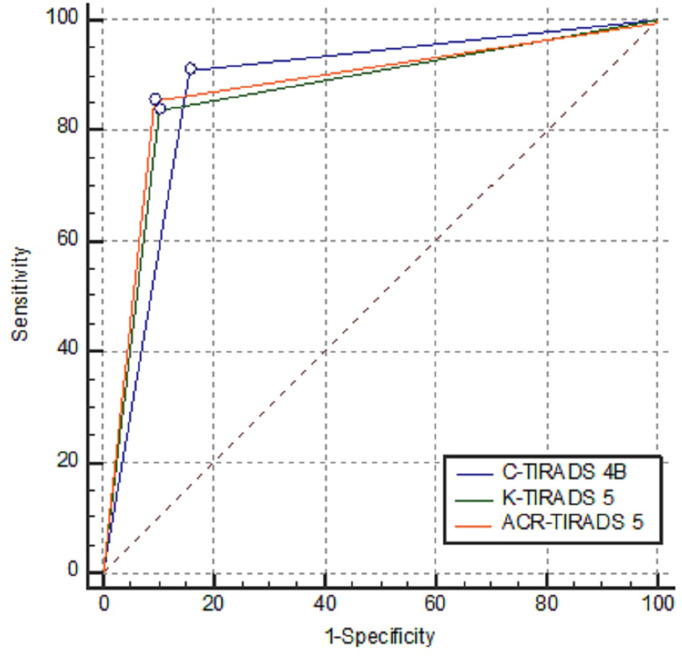
The thyroid imaging reporting and data system (TIRADS) was proposed by experts for optimal ultrasound evaluation of malignancy risk of thyroid focal lesions. There are several versions of TIRADS, some of them have been validated sufficiently, and the others have not been well assessed. In this study, a recently launched Chinese version of TIRADS (C-TIRADS) for malignancy risk stratification of thyroid nodules was validated, and the performance was compared to that of the Korean TIRADS (K-TIRADS) and American College of Radiology(ACR) TIRADS (ACR-TIRADS). Archives of 2177 patients who had undergone thyroid ultrasound examination, coarse needle tissue biopsy and/or surgery were reviewed, and 1978 patients with 1982 thyroid nodules were assessed according to the three TIRADSs. The histopathology was taken as the golden standard. The results showed the 1982 thyroid nodules were consisted of 1306 benign nodules and 676 malignant nodules. The malignancy risk accounted for 1.09%, 2.14%, 10.34%, 49.28%, 88.19% and 85.29% of the total nodules that were categorised as C-TIRADS 2, 3, 4A, 4B, 4C and 5, respectively; 0.00%, 1.64%, 2.87%,18.71% and 82.22% of the total nodules that were categorised as ACR-TIRADS 1, 2, 3, 4 and 5, respectively; 0.85%, 3.27%, 24.27% and 80.96% of the total nodules that were categorised as K-TIRADS 2, 3, 4 and 5, respectively. The correlation between the category of TIRADS and percentile of malignancy was 0.94 in the C-TIRADS, 1.00 in the ACR-TIRADS, and 1.00 in the K-TIRADS, respectively. The highest values of accuracy(AUC) ROC curves C-TIRADS 4B, K-TIRADS 5 and ACR-TIRADS 5 were taken as the cut-off values for risk stratification, respectively. The sensitivity, specificity, positive and negative predictive values and AUC by C-TIRADS 4B, K-TIRADS 5 and ACR-TIRADS 5 for malignancy risk stratification of thyroid nodules were 90.83%, 84.23%, 74.88% and 94.66% and 0.88, respectively; 83.58%, 89.82%, 80.95%, 91.36% and 0.87, respectively; and 85.50%, 90.35%, 82.10%, 92.33% and 0.88, respectively (>0.05 for all). We concluded that the C-TIRADS has excellent performance in the malignancy risk stratification of thyroid nodules by the optimized cut-off value, which is comparable to that in K-TIRADS and ACR-TIRADS.
甲状腺影像报告和数据系统(TIRADS)是由专家提出的,用于优化甲状腺局灶性病变恶性风险的超声评估。目前已有多个版本的 TIRADS,其中一些已经得到充分验证,而另一些则尚未得到很好的评估。本研究验证了一种新推出的用于甲状腺结节恶性风险分层的中文版 TIRADS(C-TIRADS),并与韩国 TIRADS(K-TIRADS)和美国放射学院(ACR)TIRADS(ACR-TIRADS)进行了比较。回顾了 2177 例接受甲状腺超声检查、粗针组织活检和/或手术的患者的档案,根据三种 TIRADS 对 1978 例 1982 个甲状腺结节进行了评估。以组织病理学为金标准。结果显示,1982 个甲状腺结节中良性结节 1306 个,恶性结节 676 个。恶性风险分别为 C-TIRADS 2、3、4A、4B、4C 和 5 分类的 1.09%、2.14%、10.34%、49.28%、88.19%和 85.29%;ACR-TIRADS 1、2、3、4 和 5 分类的分别为 0.00%、1.64%、2.87%、18.71%和 82.22%;K-TIRADS 2、3、4 和 5 分类的分别为 0.85%、3.27%、24.27%和 80.96%。C-TIRADS 中 TIRADS 类别与恶性百分率之间的相关性为 0.94,ACR-TIRADS 为 1.00,K-TIRADS 为 1.00。C-TIRADS 4B、K-TIRADS 5 和 ACR-TIRADS 5 的 ROC 曲线下面积(AUC)最高值分别作为风险分层的截断值。C-TIRADS 4B、K-TIRADS 5 和 ACR-TIRADS 5 用于甲状腺结节恶性风险分层的灵敏度、特异性、阳性和阴性预测值及 AUC 分别为 90.83%、84.23%、74.88%和 94.66%及 0.88;83.58%、89.82%、80.95%、91.36%和 0.87;85.50%、90.35%、82.10%、92.33%和 0.88(均>0.05)。结论:通过优化截断值,C-TIRADS 在甲状腺结节恶性风险分层中具有优异的性能,与 K-TIRADS 和 ACR-TIRADS 相当。