Department of Hematology, Oncology, Hemostaseology and Stem Cell Transplantation, RWTH Aachen University Hospital, Pauwelsstrasse 30, 52074, Aachen, Germany.
Institute of Laboratory Medicine, Universities of Giessen and Marburg Lung Center (UGMLC), Philipps University Marburg, German Center for Lung Research (DZL) Marburg, Marburg, Germany.
BMC Cancer. 2022 Jul 6;22(1):735. doi: 10.1186/s12885-022-09775-y.
The therapeutic armamentarium in multiple myeloma has been significantly broadened by proteasome inhibitors, highly efficient means in controlling of multiple myeloma. Despite the developments of therapeutic regimen in treatment of multiple myeloma, still the complete remission requires a novel therapeutic strategy with significant difference in outcomes. Proteasome inhibitors induce autophagy and ER stress, both pivotal pathways for protein homeostasis. Recent studies showed that the IRE1α-XBP1 axis of the unfolded protein response (UPR) is up-regulated in multiple myeloma patients. In addition, XBP1 is crucial for the maintenance of viability of acute lymphoblastic leukemia (ALL).
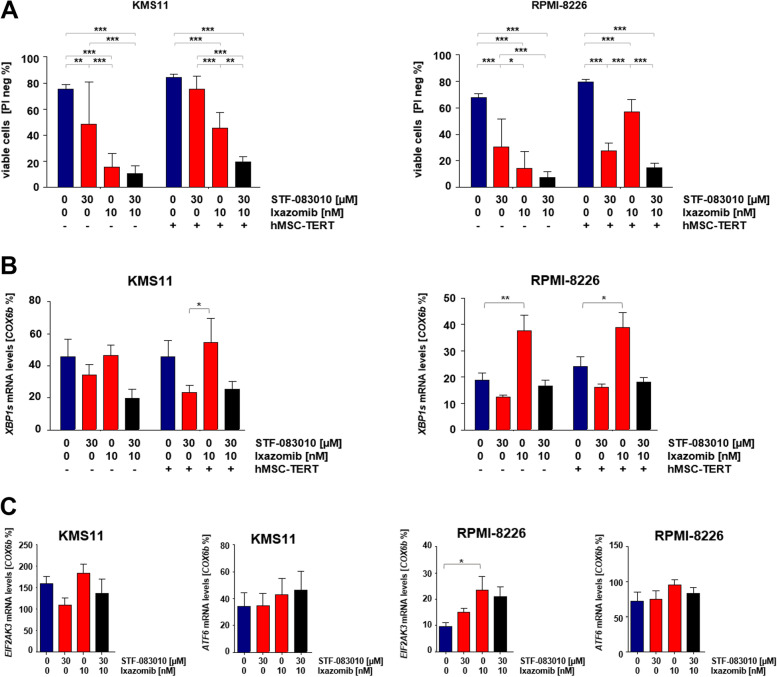
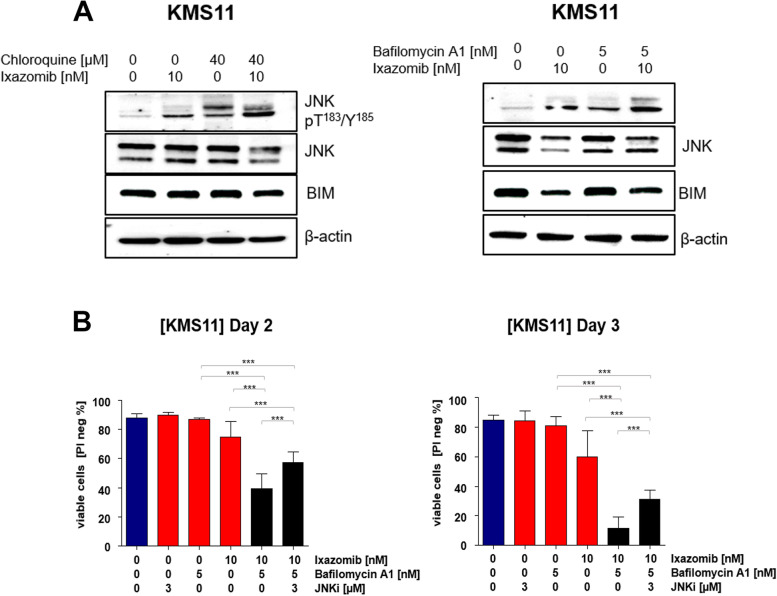
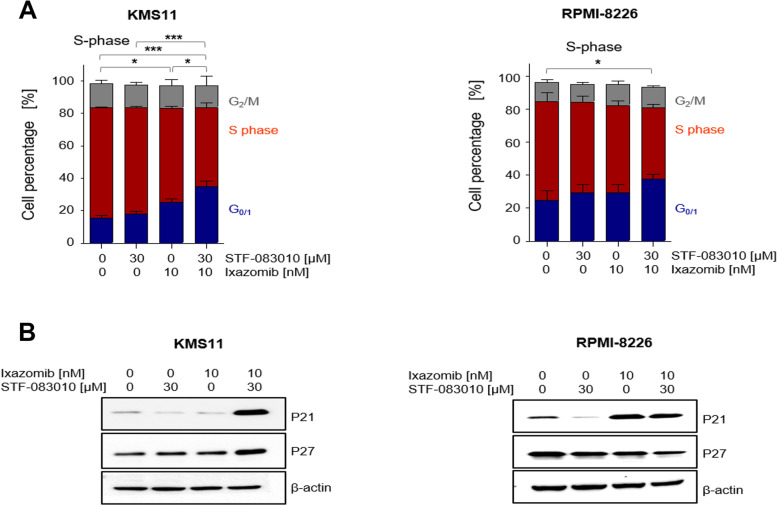
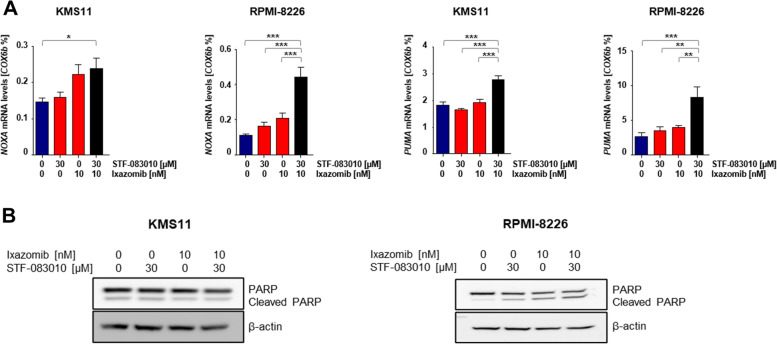
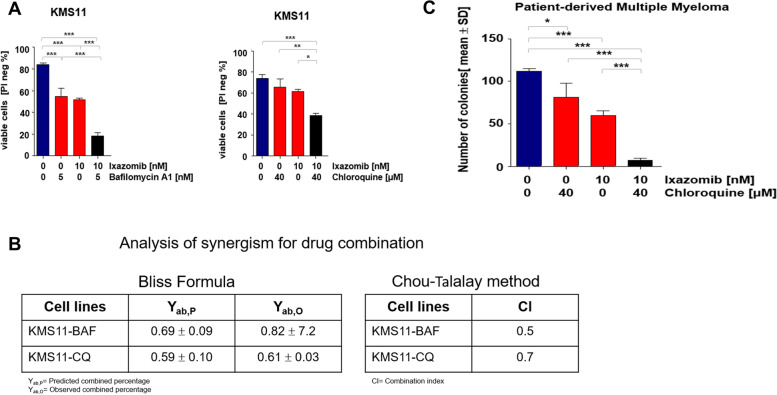
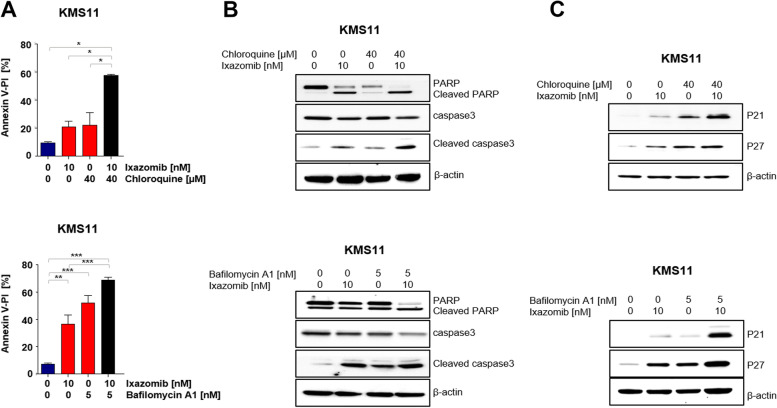
We analyzed the efficacy of targeting IRE1α-XBP1 axis and autophagy in combination with proteasome inhibitor, ixazomib in treatment of multiple myeloma. In this present study, we first show that targeting the IRE1α-XBP1 axis with small molecule inhibitors (STF-083010, A106) together with the ixazomib induces cell cycle arrest with an additive cytotoxic effect in multiple myeloma. Further, we examined the efficacy of autophagy inhibitors (bafilomycin A, BAF and chloroquine, CQ) together with ixazomib in multiple myeloma and observed that this combination treatment synergistically reduced cell viability in multiple myeloma cell lines (viable cells Ixa: 51.8 ± 3.3, Ixa + BAF: 18.3 ± 7.2, Ixa + CQ: 38.4 ± 3.7) and patient-derived multiple myeloma cells (Ixa: 59.6 ± 4.4, Ixa + CQ: 7.0 ± 2.1). We observed, however, that this combined strategy leads to activation of stress-induced c-Jun N-terminal kinase (JNK). Cytotoxicity mediated by combined proteasome and autophagy inhibition was reversed by addition of the specific JNK inhibitor JNK-In-8 (viable cells: Ixa + BAF: 11.6 ± 7.0, Ixa + BAF + JNK-In-8: 30.9 ± 6.1).
In this study we showed that combined inhibition of autophagy and the proteasome synergistically induces cell death in multiple myeloma. Hence, we consider the implication of pharmaceutical inhibition of autophagy together with proteasome inhibition and UPR-directed therapy as promising novel in vitro treatment strategy against multiple myeloma.
蛋白酶体抑制剂显著拓宽了多发性骨髓瘤的治疗手段,是控制多发性骨髓瘤的高效手段。尽管多发性骨髓瘤的治疗方案有所发展,但完全缓解仍需要一种具有显著差异疗效的新治疗策略。蛋白酶体抑制剂诱导自噬和内质网应激,这两者都是蛋白质动态平衡的关键途径。最近的研究表明, unfolded protein response(UPR)的IRE1α-XBP1 轴在多发性骨髓瘤患者中上调。此外,XBP1 对急性淋巴细胞白血病(ALL)的存活至关重要。
我们分析了靶向 IRE1α-XBP1 轴和自噬与蛋白酶体抑制剂依沙佐米联合治疗多发性骨髓瘤的疗效。在本研究中,我们首先表明,用小分子抑制剂(STF-083010、A106)靶向 IRE1α-XBP1 轴与依沙佐米联合使用,可诱导多发性骨髓瘤细胞周期停滞,并具有附加的细胞毒性作用。此外,我们研究了自噬抑制剂(巴弗洛霉素 A、BAF 和氯喹、CQ)与依沙佐米联合治疗多发性骨髓瘤的疗效,观察到这种联合治疗可协同降低多发性骨髓瘤细胞系(存活细胞 Ixa:51.8±3.3,Ixa+BAF:18.3±7.2,Ixa+CQ:38.4±3.7)和患者来源的多发性骨髓瘤细胞(Ixa:59.6±4.4,Ixa+CQ:7.0±2.1)的活力。然而,我们观察到,这种联合策略会导致应激诱导的 c-Jun N 末端激酶(JNK)的激活。用特异性 JNK 抑制剂 JNK-In-8 (存活细胞:Ixa+BAF:11.6±7.0,Ixa+BAF+JNK-In-8:30.9±6.1)可以逆转联合蛋白酶体和自噬抑制引起的细胞毒性。
在这项研究中,我们表明,自噬和蛋白酶体的联合抑制协同诱导多发性骨髓瘤细胞死亡。因此,我们认为,与蛋白酶体抑制和 UPR 定向治疗一起抑制自噬的药物抑制可能是一种很有前途的多发性骨髓瘤新型体外治疗策略。