Department of Sociology, University of Minnesota, Minneapolis.
Minnesota Population Center, University of Minnesota, Minneapolis.
JAMA Netw Open. 2022 Jul 1;5(7):e2219672. doi: 10.1001/jamanetworkopen.2022.19672.
Identifying modifiable risk factors that are associated with dementia burden across racial and ethnic groups in the population can yield insights into the potential effectiveness of interventions in preventing dementia and reducing disparities.
To calculate the population attributable fraction (PAF) of dementia associated with 12 established modifiable risk factors for all US adults, as well as separately by race and ethnicity.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study used survey data from nationally representative samples of US adults. PAFs were calculated using relative risks and prevalence estimates for 12 risk factors. Relative risks were taken from meta-analyses, as reported in a 2020 systematic review. Prevalence estimates for risk factors were derived from nationally representative cross-sectional survey data collected between 2011 and 2018. Combined PAFs were adjusted for risk factor communality using weights derived from the Atherosclerosis Risk in Communities (ARIC) study (1987-2018). Analyses were conducted May through October 2021.
Low education, hearing loss, traumatic brain injury, hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution.
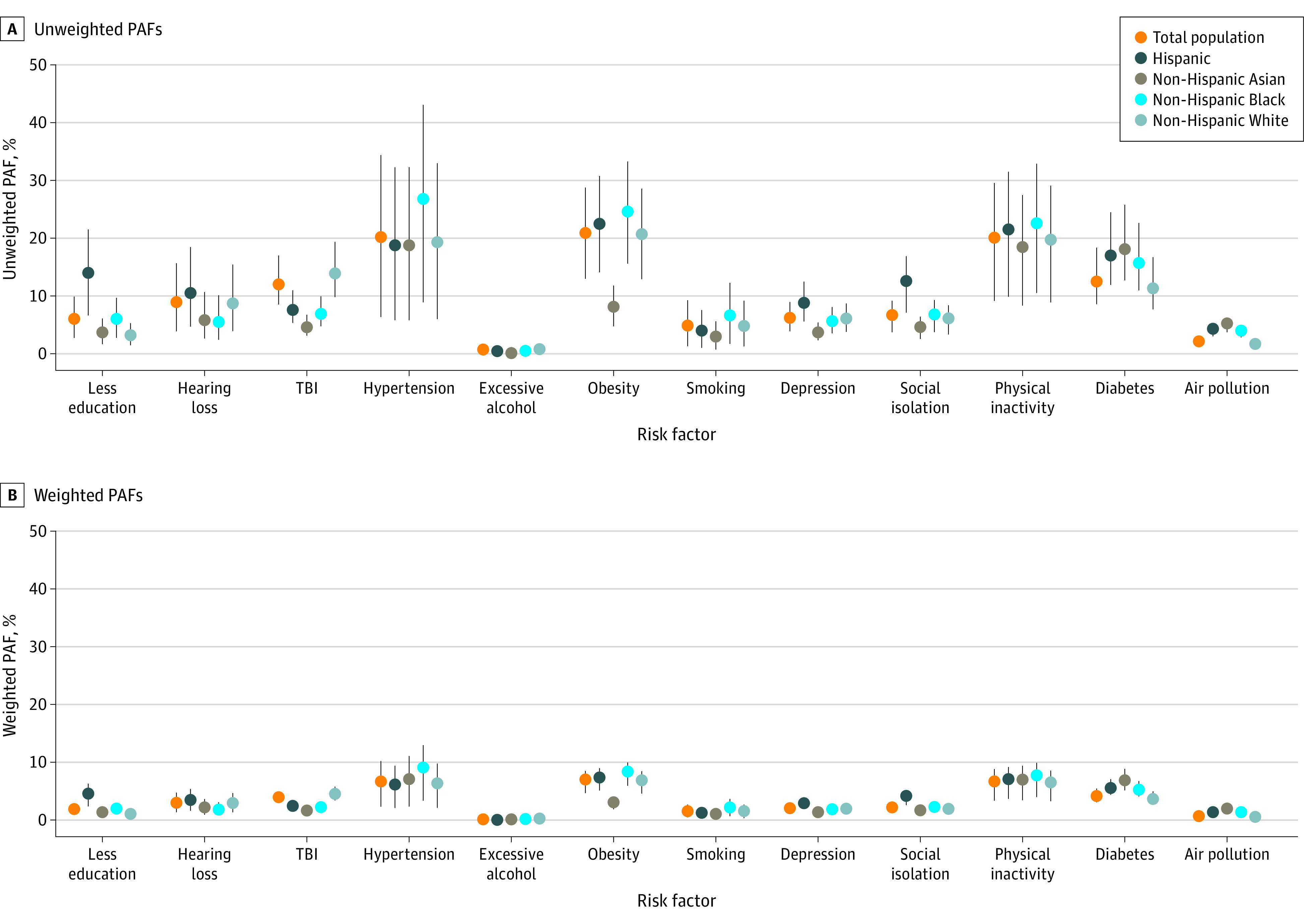
PAF for each dementia risk factor, a combined PAF, and the decrease in the number of prevalent dementia cases in 2020 that would be expected given a 15% proportional decrease in each exposure.
Among all US adults, an estimated 41.0% (95% CI, 22.7%-55.9%) of dementia cases were attributable to 12 risk factors. A 15% proportional decrease in each risk factor would reduce dementia prevalence in the population by an estimated 7.3% (95% CI, 3.7%-10.9%). The estimated PAF was greater for Black and Hispanic than it was for White and Asian individuals. The greatest attributable fraction of dementia cases was observed for hypertension (PAF, 20.2%; 95% CI, 6.3%-34.4%), obesity (PAF, 20.9%; 95% CI, 13.0%-28.8%), and physical inactivity (PAF, 20.1%; 95% CI, 9.1%-29.6%). These factors were also highest within each racial and ethnic group, although the proportions varied.
A large fraction of dementia cases in the US were associated with potentially modifiable risk factors, especially for Black and Hispanic individuals. Targeting and reducing these risk factors may curb the projected rise in dementia cases over the next several decades.
确定与人群中不同种族和族裔的痴呆负担相关的可改变风险因素,可以深入了解预防痴呆和减少差异的干预措施的潜在有效性。
计算与所有美国成年人的 12 种既定可改变风险因素相关的痴呆的人群归因分数 (PAF),并按种族和族裔分别计算。
设计、设置和参与者:这项横断面研究使用了来自具有全国代表性的美国成年人样本的调查数据。使用 12 个风险因素的相对风险和流行率估计值计算 PAF。相对风险来自于 2020 年系统评价中报告的荟萃分析。风险因素的流行率估计值来自于 2011 年至 2018 年期间收集的具有全国代表性的横断面调查数据。使用从动脉粥样硬化风险社区研究 (ARIC) (1987-2018) 中得出的权重对风险因素的共同性进行了调整。分析于 2021 年 5 月至 10 月进行。
低教育水平、听力损失、创伤性脑损伤、高血压、过量饮酒、肥胖、吸烟、抑郁、社会孤立、身体活动不足、糖尿病和空气污染。
每个痴呆风险因素的 PAF、综合 PAF 以及在每种暴露减少 15%的情况下,预计 2020 年将出现的常见痴呆病例数的减少。
在美国所有成年人中,估计有 41.0%(95%CI,22.7%-55.9%)的痴呆病例归因于 12 个风险因素。每种风险因素减少 15%,预计将使人群中的痴呆患病率降低约 7.3%(95%CI,3.7%-10.9%)。与白人和亚洲人相比,黑人和西班牙裔的估计 PAF 更高。高血压(PAF,20.2%;95%CI,6.3%-34.4%)、肥胖症(PAF,20.9%;95%CI,13.0%-28.8%)和身体活动不足(PAF,20.1%;95%CI,9.1%-29.6%)导致的痴呆病例比例最高。这些因素在每个种族和族裔群体中也是最高的,尽管比例有所不同。
美国很大一部分痴呆病例与潜在的可改变风险因素有关,尤其是黑人和西班牙裔人群。针对这些风险因素并加以减少,可能会遏制未来几十年痴呆病例的预计上升。